{"title":"Mean arterial pressure at the initiation of continuous renal replacement therapy as a prognostic indicator in patients with acute kidney injury.","authors":"Haiying Song, Yuheng Liao, Haofei Hu, Qijun Wan","doi":"10.1080/0886022X.2024.2448582","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) is a common complication in critically ill patients, with approximately 5% requiring continuous renal replacement therapy (CRRT). This study investigated the relationship between mean arterial pressure (MAP) and 28- and 90-day mortality in critically ill AKI patients treated with CRRT.</p><p><strong>Methods: </strong>This secondary analysis of a bicenter, retrospective, observational study included patients with AKI who were treated with CRRT from January 2009 to September 2016. Mortality at 28 and 90 days post-CRRT initiation was analyzed using multivariate regression, generalized additive models, smooth curve fitting, and sensitivity analyses.</p><p><strong>Results: </strong>A total of 1,142 patients were included, with 28-day and 90-day mortality rates of 62.1% and 71.8%, respectively. In multivariable-adjusted Cox models, MAP was inversely correlated with the risk of 28-day and 90-day mortality after adjusting for covariates. Hazard ratios (HRs) were calculated per 1 mmHg increment of MAP: adjusted HR for 28-day mortality 0.985 (<i>p</i> < 0.00001) and for 90-day mortality 0.987 (<i>p</i> = 0.00002). The adjusted HRs for 28-day and 90-day mortality in patients in the highest tertile of MAP compared with those in the lowest tertile were 0.682 (95% CI 0.543-0.857) and 0.730 (95% CI 0.592-0.899), respectively. Patients were grouped using MAP thresholds of <65 mmHg, 65-71.85 mmHg, and ≥71.85 mmHg, with similar results observed. Sensitivity analyses confirmed the inverse relationship between higher MAP before CRRT and lower mortality.</p><p><strong>Conclusion: </strong>The higher the MAP before CRRT is, the lower the 28- and 90-day mortality of critically ill patients with AKI who are treated with CRRT.</p>","PeriodicalId":20839,"journal":{"name":"Renal Failure","volume":"47 1","pages":"2448582"},"PeriodicalIF":3.0000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11721759/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Renal Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/0886022X.2024.2448582","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute kidney injury (AKI) is a common complication in critically ill patients, with approximately 5% requiring continuous renal replacement therapy (CRRT). This study investigated the relationship between mean arterial pressure (MAP) and 28- and 90-day mortality in critically ill AKI patients treated with CRRT.
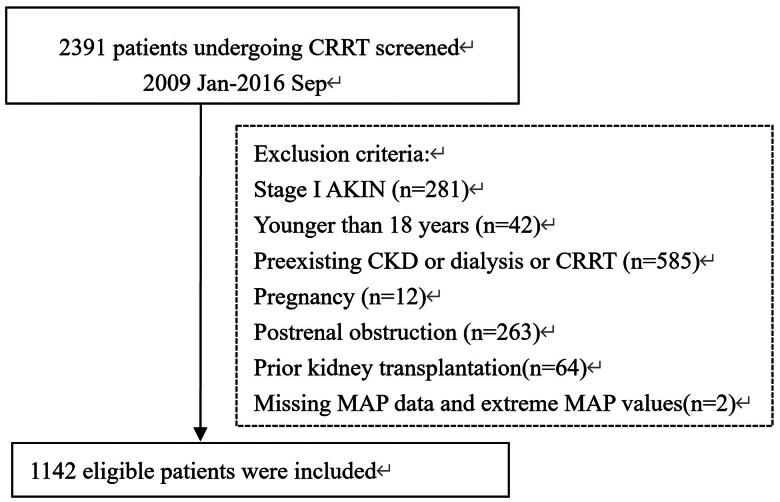
Methods: This secondary analysis of a bicenter, retrospective, observational study included patients with AKI who were treated with CRRT from January 2009 to September 2016. Mortality at 28 and 90 days post-CRRT initiation was analyzed using multivariate regression, generalized additive models, smooth curve fitting, and sensitivity analyses.
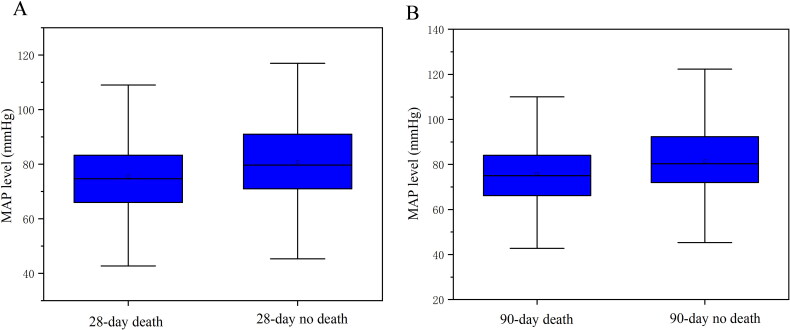
Results: A total of 1,142 patients were included, with 28-day and 90-day mortality rates of 62.1% and 71.8%, respectively. In multivariable-adjusted Cox models, MAP was inversely correlated with the risk of 28-day and 90-day mortality after adjusting for covariates. Hazard ratios (HRs) were calculated per 1 mmHg increment of MAP: adjusted HR for 28-day mortality 0.985 (p < 0.00001) and for 90-day mortality 0.987 (p = 0.00002). The adjusted HRs for 28-day and 90-day mortality in patients in the highest tertile of MAP compared with those in the lowest tertile were 0.682 (95% CI 0.543-0.857) and 0.730 (95% CI 0.592-0.899), respectively. Patients were grouped using MAP thresholds of <65 mmHg, 65-71.85 mmHg, and ≥71.85 mmHg, with similar results observed. Sensitivity analyses confirmed the inverse relationship between higher MAP before CRRT and lower mortality.
Conclusion: The higher the MAP before CRRT is, the lower the 28- and 90-day mortality of critically ill patients with AKI who are treated with CRRT.
背景:急性肾损伤(AKI)是危重患者的常见并发症,约5%的患者需要持续肾替代治疗(CRRT)。本研究探讨了接受CRRT治疗的危重AKI患者的平均动脉压(MAP)与28天和90天死亡率之间的关系。方法:本研究对2009年1月至2016年9月期间接受CRRT治疗的AKI患者进行了一项双中心、回顾性、观察性研究。采用多元回归、广义加性模型、平滑曲线拟合和敏感性分析对crrt开始后28天和90天的死亡率进行分析。结果:共纳入1142例患者,28天和90天死亡率分别为62.1%和71.8%。在多变量校正Cox模型中,经协变量校正后,MAP与28天和90天死亡率呈负相关。MAP每增加1 mmHg计算危险比(HR):调整后28天死亡率HR为0.985 (p p = 0.00002)。MAP最高分位患者与最低分位患者的28天和90天死亡率调整hr分别为0.682 (95% CI 0.543-0.857)和0.730 (95% CI 0.592-0.899)。结论:CRRT前MAP越高,行CRRT治疗的AKI危重患者28天和90天死亡率越低。
期刊介绍:
Renal Failure primarily concentrates on acute renal injury and its consequence, but also addresses advances in the fields of chronic renal failure, hypertension, and renal transplantation. Bringing together both clinical and experimental aspects of renal failure, this publication presents timely, practical information on pathology and pathophysiology of acute renal failure; nephrotoxicity of drugs and other substances; prevention, treatment, and therapy of renal failure; renal failure in association with transplantation, hypertension, and diabetes mellitus.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
