Optimising fatigue, abdominal pain and faecal incontinence in people with inflammatory bowel disease (IBD-BOOST Optimise): feasibility study of a checklist and algorithm for initial nurse-led management.
Imogen Stagg, Ailsa Hart, Fionn Cléirigh Büttner, Asma Fikree, John McLaughlin, Jean-Frederic LeBlanc, Sonia Bouri, Thomas Hamborg, Laura Miller, Christine Norton
{"title":"Optimising fatigue, abdominal pain and faecal incontinence in people with inflammatory bowel disease (IBD-BOOST Optimise): feasibility study of a checklist and algorithm for initial nurse-led management.","authors":"Imogen Stagg, Ailsa Hart, Fionn Cléirigh Büttner, Asma Fikree, John McLaughlin, Jean-Frederic LeBlanc, Sonia Bouri, Thomas Hamborg, Laura Miller, Christine Norton","doi":"10.1136/bmjgast-2024-001585","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Many people with inflammatory bowel disease (IBD) experience fatigue, pain and faecal incontinence that some feel are inadequately addressed. It is unknown how many have potentially reversible medical issues underlying these symptoms.</p><p><strong>Methods: </strong>We conducted a study testing the feasibility of a patient-reported symptom checklist and nurse-administered management algorithm ('Optimise') to manage common medical causes of IBD-related fatigue, pain and faecal incontinence. We conducted qualitative interviews with nurses implementing the algorithm.</p><p><strong>Results: </strong>515 individuals reporting IBD-related symptoms were invited to participate, of whom 201 (39%) consented. 194/201 (97%) returned the symptom checklist, of whom 157 (81%) returned a postal faecal calprotectin sample. Five (3%) participants reported 'red flags' and 31/157 (20%) participants had a faecal calprotectin result ≥200 µg/g, of whom 12 (8%) were judged to have likely active inflammation when clinical symptoms and disease history were reviewed. The algorithm suggested at least one clinical test or intervention for fatigue, pain or faecal incontinence in 67 (43%) participants, of whom 25 (37%) declined. Among 87 participants for whom clinical actions were indicated, 57 (66%) completed follow-up outcomes 3 months after algorithm implementation. Three nurses interviewed found the Optimise algorithm easy to administer.</p><p><strong>Conclusion: </strong>Implementing the Optimise checklist and algorithm appears feasible in UK clinical practice, with adjustments needed to minimise missing items. Not all patients accepted algorithm-indicated interventions, but a yield of 43% with symptoms having potentially reversible causes detected is clinically useful. Nurses endorsed ease and utility of the implementation process. Optimise now needs clinical effectiveness to be assessed.</p>","PeriodicalId":9235,"journal":{"name":"BMJ Open Gastroenterology","volume":"11 1","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11664377/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjgast-2024-001585","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Many people with inflammatory bowel disease (IBD) experience fatigue, pain and faecal incontinence that some feel are inadequately addressed. It is unknown how many have potentially reversible medical issues underlying these symptoms.
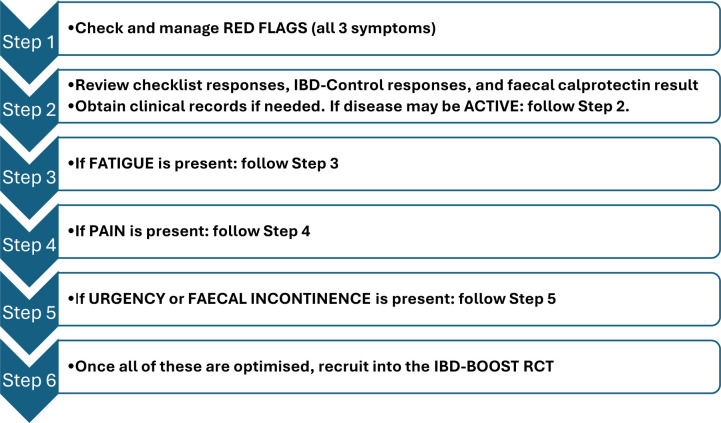
Methods: We conducted a study testing the feasibility of a patient-reported symptom checklist and nurse-administered management algorithm ('Optimise') to manage common medical causes of IBD-related fatigue, pain and faecal incontinence. We conducted qualitative interviews with nurses implementing the algorithm.
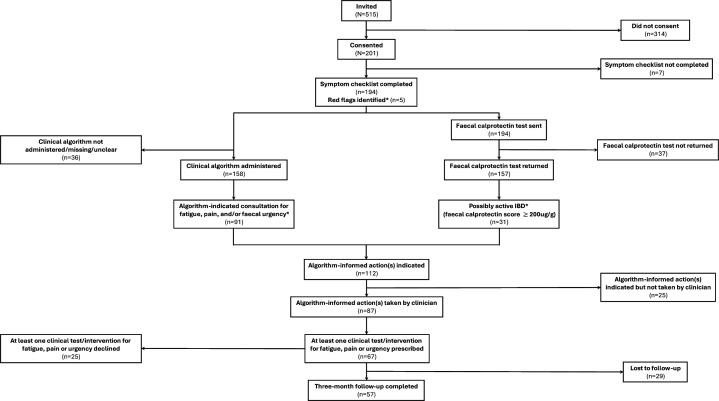
Results: 515 individuals reporting IBD-related symptoms were invited to participate, of whom 201 (39%) consented. 194/201 (97%) returned the symptom checklist, of whom 157 (81%) returned a postal faecal calprotectin sample. Five (3%) participants reported 'red flags' and 31/157 (20%) participants had a faecal calprotectin result ≥200 µg/g, of whom 12 (8%) were judged to have likely active inflammation when clinical symptoms and disease history were reviewed. The algorithm suggested at least one clinical test or intervention for fatigue, pain or faecal incontinence in 67 (43%) participants, of whom 25 (37%) declined. Among 87 participants for whom clinical actions were indicated, 57 (66%) completed follow-up outcomes 3 months after algorithm implementation. Three nurses interviewed found the Optimise algorithm easy to administer.
Conclusion: Implementing the Optimise checklist and algorithm appears feasible in UK clinical practice, with adjustments needed to minimise missing items. Not all patients accepted algorithm-indicated interventions, but a yield of 43% with symptoms having potentially reversible causes detected is clinically useful. Nurses endorsed ease and utility of the implementation process. Optimise now needs clinical effectiveness to be assessed.
期刊介绍:
BMJ Open Gastroenterology is an online-only, peer-reviewed, open access gastroenterology journal, dedicated to publishing high-quality medical research from all disciplines and therapeutic areas of gastroenterology. It is the open access companion journal of Gut and is co-owned by the British Society of Gastroenterology. The journal publishes all research study types, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Publishing procedures are built around continuous publication, publishing research online as soon as the article is ready.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
