Brian K. Mitchell MD , Anna Tomdio MD , Muhammad S. Pir MD , Suraj K. Mishra MD , Pradeep Dayanand MD , Guillaume Bonnet MD, PhD , Maria C. Alu MS , Zachary M. Gertz MD
{"title":"A Randomized Trial of Cardiac Catheterization With Fasting Versus Liberal Oral Intake: The CALORI Trial","authors":"Brian K. Mitchell MD , Anna Tomdio MD , Muhammad S. Pir MD , Suraj K. Mishra MD , Pradeep Dayanand MD , Guillaume Bonnet MD, PhD , Maria C. Alu MS , Zachary M. Gertz MD","doi":"10.1016/j.jscai.2024.102291","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Routine preprocedural fasting before cardiac catheterization remains common practice, despite a lack of robust evidence to support this practice. We investigated the impact of a liberal nonfasting strategy vs a standardized nil per os (NPO) regimen prior to cardiac catheterization.</div></div><div><h3>Methods</h3><div>Adult inpatients undergoing elective or urgent cardiac catheterization were randomized (1:1 ratio) to either NPO past midnight or ad libitum intake of liquids and solids (without dietary constraints) until immediately prior to the procedure. Only patients at high risk of aspiration or undergoing complex interventions were excluded. The primary end point was preprocedural patient-reported well-being scores (scaled 0-5, with 0 signifying absence of ailment and 5 the most extreme form), for variables including hunger, fatigue, anxiety, and nausea. A composite score summed the individual scores for hunger and fatigue. Other end points were periprocedural adverse events including emesis, aspiration, or intubation, in addition to postprocedural satisfaction.</div></div><div><h3>Results</h3><div>A total of 198 patients (65% male and 42% Black) were included in the final analysis. There were no differences in baseline characteristics between groups. Time from most recent oral intake (liquid or solid) to the start of the procedure averaged 148 minutes for the nonfasting group and 970 minutes for the NPO strategy (<em>P</em> < .001). The composite preprocedural well-being score was significantly better in the nonfasting arm (2.4 ± 2.4 nonfasting vs 6.0 ± 2.5 NPO; <em>P</em> < .001), as were the individual components of hunger (0.9 ± 1.5 vs 3.7 ± 1.5; <em>P</em> < .001), fatigue (1.5 ± 1.6 vs 2.3 ± 1.8; <em>P</em> < .001), and nausea (0.1 ± 0.5 vs 0.5 ±1.2; <em>P</em> = .006). There were no significant differences in adverse events between groups. Overall postprocedural satisfaction scores were significantly better in the nonfasting vs NPO group (0.3 ± 0.7 vs 1.0 ± 1.3, respectively; <em>P</em> < .001).</div></div><div><h3>Conclusions</h3><div>In this single-center randomized trial, a liberal nonfasting strategy prior to cardiac catheterization significantly improved patient well-being and satisfaction without compromising safety. Given the findings of this and other studies, routine fasting prior to cardiac catheterization should be reconsidered.</div></div>","PeriodicalId":73990,"journal":{"name":"Journal of the Society for Cardiovascular Angiography & Interventions","volume":"3 12","pages":"Article 102291"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11725108/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Society for Cardiovascular Angiography & Interventions","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772930324017356","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Routine preprocedural fasting before cardiac catheterization remains common practice, despite a lack of robust evidence to support this practice. We investigated the impact of a liberal nonfasting strategy vs a standardized nil per os (NPO) regimen prior to cardiac catheterization.
Methods
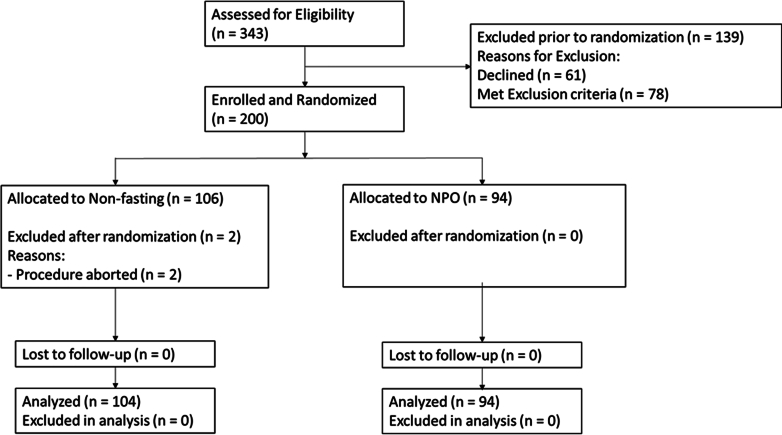
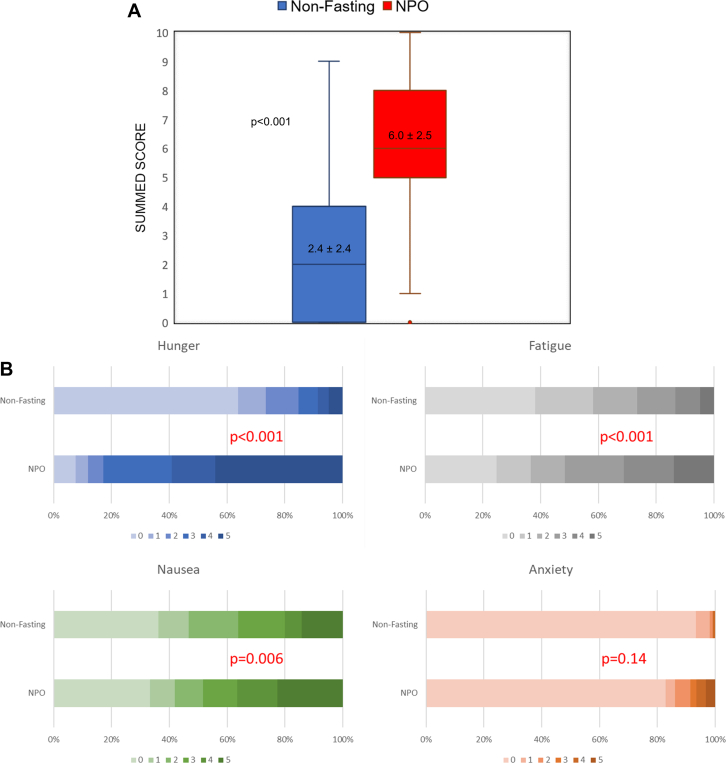
Adult inpatients undergoing elective or urgent cardiac catheterization were randomized (1:1 ratio) to either NPO past midnight or ad libitum intake of liquids and solids (without dietary constraints) until immediately prior to the procedure. Only patients at high risk of aspiration or undergoing complex interventions were excluded. The primary end point was preprocedural patient-reported well-being scores (scaled 0-5, with 0 signifying absence of ailment and 5 the most extreme form), for variables including hunger, fatigue, anxiety, and nausea. A composite score summed the individual scores for hunger and fatigue. Other end points were periprocedural adverse events including emesis, aspiration, or intubation, in addition to postprocedural satisfaction.
Results
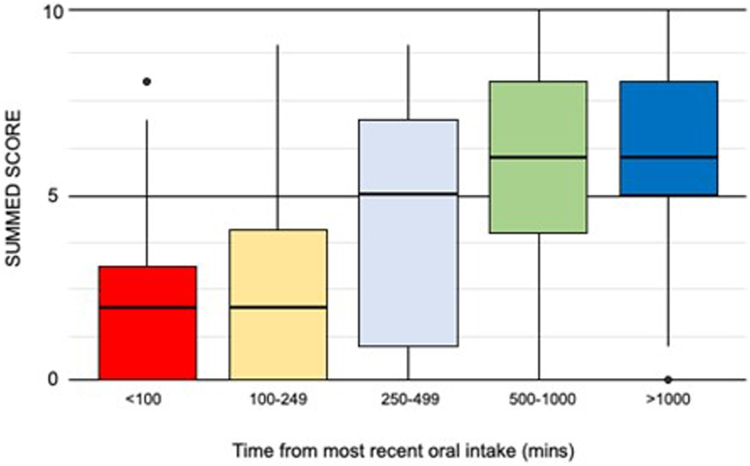
A total of 198 patients (65% male and 42% Black) were included in the final analysis. There were no differences in baseline characteristics between groups. Time from most recent oral intake (liquid or solid) to the start of the procedure averaged 148 minutes for the nonfasting group and 970 minutes for the NPO strategy (P < .001). The composite preprocedural well-being score was significantly better in the nonfasting arm (2.4 ± 2.4 nonfasting vs 6.0 ± 2.5 NPO; P < .001), as were the individual components of hunger (0.9 ± 1.5 vs 3.7 ± 1.5; P < .001), fatigue (1.5 ± 1.6 vs 2.3 ± 1.8; P < .001), and nausea (0.1 ± 0.5 vs 0.5 ±1.2; P = .006). There were no significant differences in adverse events between groups. Overall postprocedural satisfaction scores were significantly better in the nonfasting vs NPO group (0.3 ± 0.7 vs 1.0 ± 1.3, respectively; P < .001).
Conclusions
In this single-center randomized trial, a liberal nonfasting strategy prior to cardiac catheterization significantly improved patient well-being and satisfaction without compromising safety. Given the findings of this and other studies, routine fasting prior to cardiac catheterization should be reconsidered.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
