Natalie Kreitzer, Nancy M Albert, Alpesh N Amin, Craig J Beavers, Richard C Becker, Gregg Fonarow, W Brian Gibler, Katherine W Kwon, Robert J Mentz, Biff F Palmer, Charles V Pollack, Ileana L Piña
{"title":"EMCREG-International Multidisciplinary Consensus Panel on Management of Hyperkalemia in Chronic Kidney Disease and Heart Failure.","authors":"Natalie Kreitzer, Nancy M Albert, Alpesh N Amin, Craig J Beavers, Richard C Becker, Gregg Fonarow, W Brian Gibler, Katherine W Kwon, Robert J Mentz, Biff F Palmer, Charles V Pollack, Ileana L Piña","doi":"10.1159/000543385","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hyperkalemia, generally defined as serum potassium levels greater than 5.0 mEq/L, poses significant clinical risks, including cardiac toxicity and muscle weakness. Its prevalence and severity increase in patients with chronic kidney disease (CKD), diabetes mellitus, and heart failure (HF), particularly when compounded by medications like angiotensin converting inhibitors, angiotensin receptor blockers, and potassium sparing diuretics. Hyperkalemia arises from disruptions in potassium regulation involving intake, excretion, and intracellular-extracellular distribution. In CKD and acute kidney injury, these regulatory mechanisms are impaired, leading to heightened risk. The management of chronic hyperkalemia presents a challenge due to the necessity of balancing effective cardiovascular and renal therapies against the risk of elevated potassium levels.</p><p><strong>Summary: </strong>The emergency department management of acute hyperkalemia focuses on preventing cardiac complications through strategies that stabilize cellular membranes and shift potassium intracellularly. Chronic management often involves dietary interventions and pharmacological treatments. Pharmacological management of acute hyperkalemia includes diuretics, which enhance kaliuresis, and potassium binders such as patiromer and sodium zirconium cyclosilicate, which facilitate fecal excretion of potassium. While diuretics are commonly used, they carry risks of volume contraction and renal function deterioration. The newer potassium binders have shown efficacy in lowering chronically elevated potassium levels in CKD and HF patients, offering an alternative to diuretics and other older agents such as sodium polystyrene sulfonate, which has significant adverse effects and limited evidence for chronic use.</p><p><strong>Key messages: </strong>We convened a consensus panel to describe the optimal management across multiple clinical settings when caring for patients with hyperkalemia. This consensus emphasizes a multidisciplinary approach to managing hyperkalemia, particularly in patients with cardiovascular kidney metabolic syndrome, to avoid fragmentation of care and ensure comprehensive treatment strategies. The primary goal of this manuscript is to describe strategies to maintain cardiovascular benefits of essential medications while effectively managing potassium levels.</p>","PeriodicalId":9584,"journal":{"name":"Cardiorenal Medicine","volume":" ","pages":"133-152"},"PeriodicalIF":2.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11844669/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiorenal Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000543385","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
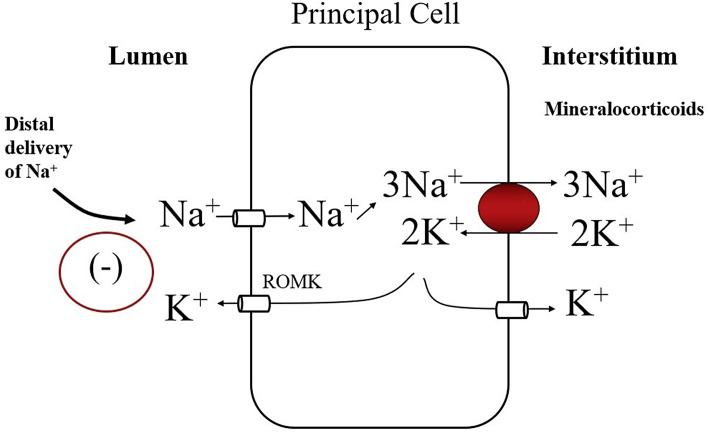
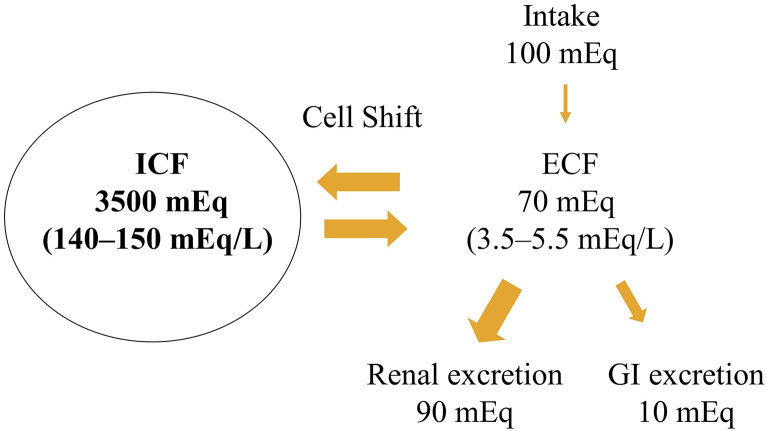
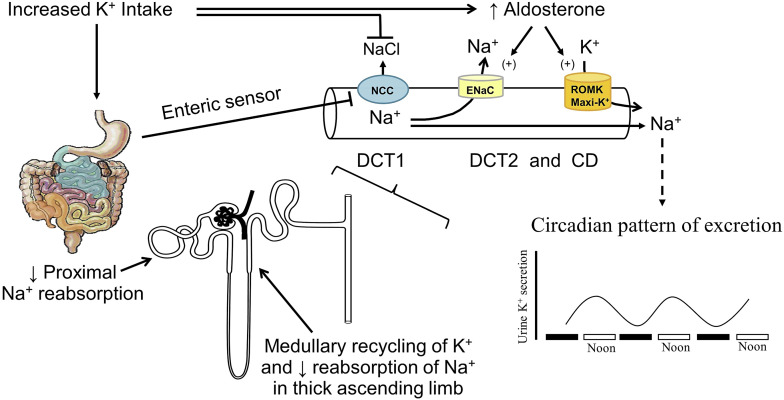
Background: Hyperkalemia, generally defined as serum potassium levels greater than 5.0 mEq/L, poses significant clinical risks, including cardiac toxicity and muscle weakness. Its prevalence and severity increase in patients with chronic kidney disease (CKD), diabetes mellitus, and heart failure (HF), particularly when compounded by medications like angiotensin converting inhibitors, angiotensin receptor blockers, and potassium sparing diuretics. Hyperkalemia arises from disruptions in potassium regulation involving intake, excretion, and intracellular-extracellular distribution. In CKD and acute kidney injury, these regulatory mechanisms are impaired, leading to heightened risk. The management of chronic hyperkalemia presents a challenge due to the necessity of balancing effective cardiovascular and renal therapies against the risk of elevated potassium levels.
Summary: The emergency department management of acute hyperkalemia focuses on preventing cardiac complications through strategies that stabilize cellular membranes and shift potassium intracellularly. Chronic management often involves dietary interventions and pharmacological treatments. Pharmacological management of acute hyperkalemia includes diuretics, which enhance kaliuresis, and potassium binders such as patiromer and sodium zirconium cyclosilicate, which facilitate fecal excretion of potassium. While diuretics are commonly used, they carry risks of volume contraction and renal function deterioration. The newer potassium binders have shown efficacy in lowering chronically elevated potassium levels in CKD and HF patients, offering an alternative to diuretics and other older agents such as sodium polystyrene sulfonate, which has significant adverse effects and limited evidence for chronic use.
Key messages: We convened a consensus panel to describe the optimal management across multiple clinical settings when caring for patients with hyperkalemia. This consensus emphasizes a multidisciplinary approach to managing hyperkalemia, particularly in patients with cardiovascular kidney metabolic syndrome, to avoid fragmentation of care and ensure comprehensive treatment strategies. The primary goal of this manuscript is to describe strategies to maintain cardiovascular benefits of essential medications while effectively managing potassium levels.
期刊介绍:
The journal ''Cardiorenal Medicine'' explores the mechanisms by which obesity and other metabolic abnormalities promote the pathogenesis and progression of heart and kidney disease (cardiorenal metabolic syndrome). It provides an interdisciplinary platform for the advancement of research and clinical practice, focussing on translational issues.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
