{"title":"A Case of IgA Nephropathy in a Patient With Sarcoidosis: Confirmation of Glomerular Galactose-Deficient IgA1 Deposition.","authors":"Yoshitaka Shimizu, Daisuke Ito, Mayumi Arakawa, Yuriko Shiozaki, Yumiko Suzuki, Seigo Ito, Naro Ohashi, Yoshihide Fujigaki, Akira Shimizu, Hideo Yasuda, Taro Misaki","doi":"10.1155/crin/7366501","DOIUrl":null,"url":null,"abstract":"<p><p>A 63-year-old Japanese housewife was admitted to our hospital because of hematuria and proteinuria lasting for 3 months. At the age of 59 years, she was diagnosed with neurosarcoidosis at another hospital, and she received oral glucocorticoid therapy for 1 year. Her serum angiotensin-converting enzyme (ACE) and 1, 25-dihydroxyvitamin D levels were elevated. Computed tomography showed lymphadenopathy of the tracheal bifurcation and diffuse nodular shadow in the lungs and liver. Renal biopsy findings were compatible with IgA nephropathy without noncaseating granulomas and glomerular galactose-deficient IgA1 (Gd-IgA1) was stained in mesangial area. Because of clinical suspicion of sarcoidosis, liver biopsy was also performed, which showed inflammation with multiple noncaseating granulomas. The patient was diagnosed with IgA nephropathy coincident with sarcoidosis. After oral administration of prednisolone, mild proteinuria persisted; however, serum creatinine level was normalized, hematuria disappeared, and serum ACE and 1, 25-dihydroxyvitamin D levels returned to normal. Although some patients with sarcoidosis occasionally present with glomerulonephritis, there have been few case reports of sarcoidosis with IgA nephropathy. This was the first case report in which glomerular Gd-IgA1 was identified in a patient with IgA nephropathy and sarcoidosis.</p>","PeriodicalId":9604,"journal":{"name":"Case Reports in Nephrology","volume":"2025 ","pages":"7366501"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11735058/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crin/7366501","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
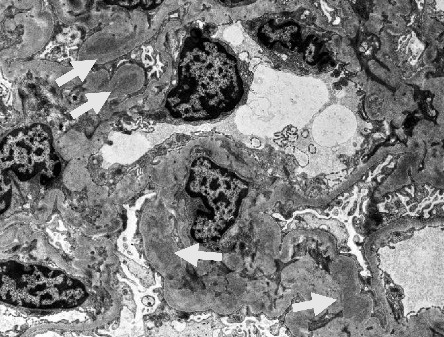
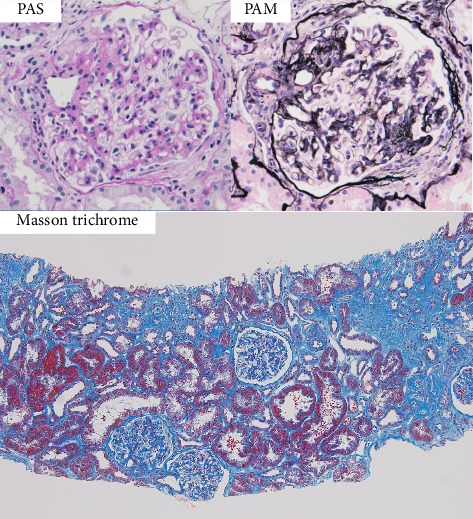
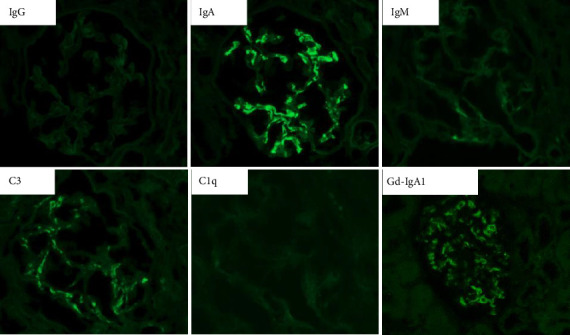
A 63-year-old Japanese housewife was admitted to our hospital because of hematuria and proteinuria lasting for 3 months. At the age of 59 years, she was diagnosed with neurosarcoidosis at another hospital, and she received oral glucocorticoid therapy for 1 year. Her serum angiotensin-converting enzyme (ACE) and 1, 25-dihydroxyvitamin D levels were elevated. Computed tomography showed lymphadenopathy of the tracheal bifurcation and diffuse nodular shadow in the lungs and liver. Renal biopsy findings were compatible with IgA nephropathy without noncaseating granulomas and glomerular galactose-deficient IgA1 (Gd-IgA1) was stained in mesangial area. Because of clinical suspicion of sarcoidosis, liver biopsy was also performed, which showed inflammation with multiple noncaseating granulomas. The patient was diagnosed with IgA nephropathy coincident with sarcoidosis. After oral administration of prednisolone, mild proteinuria persisted; however, serum creatinine level was normalized, hematuria disappeared, and serum ACE and 1, 25-dihydroxyvitamin D levels returned to normal. Although some patients with sarcoidosis occasionally present with glomerulonephritis, there have been few case reports of sarcoidosis with IgA nephropathy. This was the first case report in which glomerular Gd-IgA1 was identified in a patient with IgA nephropathy and sarcoidosis.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
