{"title":"Early Enteral Nutrition May Improve Survival in Patients With Cardiogenic Shock.","authors":"Liangliang Zheng, Jingwei Duan, Baomin Duan","doi":"10.1155/emmi/1465194","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and Aim:</b> International guidelines recommend early enteral nutrition (EEN) for critically ill patients. However, evidence supporting the optimal timing of EN in patients diagnosed with cardiogenic shock (CS) is lacking. As such, this study aimed to compare the clinical outcomes and safety of EEN versus delayed EN in patients diagnosed with CS. <b>Methods:</b> This retrospective cohort study was conducted using data from the Medical Information Mart for Intensive Care IV version 2.2 database. Patients who received EN within 2 days of admission were assigned to the EEN group. A 1:1 propensity score-matched (PSM) analysis was performed to control for bias in baseline characteristics and ensure the reliability of the results. To exclude the impact of confounders, an adjusted proportional hazards regression model was used to verify the independence between EEN and survival outcomes. <b>Results:</b> Of 1846 potentially eligible patients, 1398 received EEN and 448 received delayed EN. After 1:1 PSM, 818 patients were assigned to the EEN (<i>n</i> = 409) and delayed EN (<i>n</i> = 409) groups. Regarding cumulative survival, patients with CS receiving EEN experienced better 30-, 90-, and 180-day survival outcomes than the delayed EN group (hazard ratio [HR] 0.803 [95% confidence interval [CI] 0.647-0.998], <i>p</i>=0.045; HR 0.729 [95% CI 0.599-0.889], <i>p</i>=0.001; and HR 0.778 [95% CI 0.644-0.938], <i>p</i>=0.008, respectively). After adjusting for confounders, EEN was found to be independently associated with survival outcomes. Moreover, EEN did not increase the risk(s) for ileus, aspiration pneumonia, or gastrointestinal bleeding. Patients who received delayed EN experienced longer hospital stays than those receiving EEN (17 days [interquartile range [IQR] 10-25] versus 12 days [IQR 7-19 days], respectively; <i>p</i> < 0.001). <b>Conclusion:</b> EEN was not associated with harm, but rather with improved survival outcomes in patients diagnosed with CS. Further studies are required to verify these findings.</p>","PeriodicalId":11528,"journal":{"name":"Emergency Medicine International","volume":"2025 ","pages":"1465194"},"PeriodicalIF":0.8000,"publicationDate":"2025-01-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11729513/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Medicine International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/emmi/1465194","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
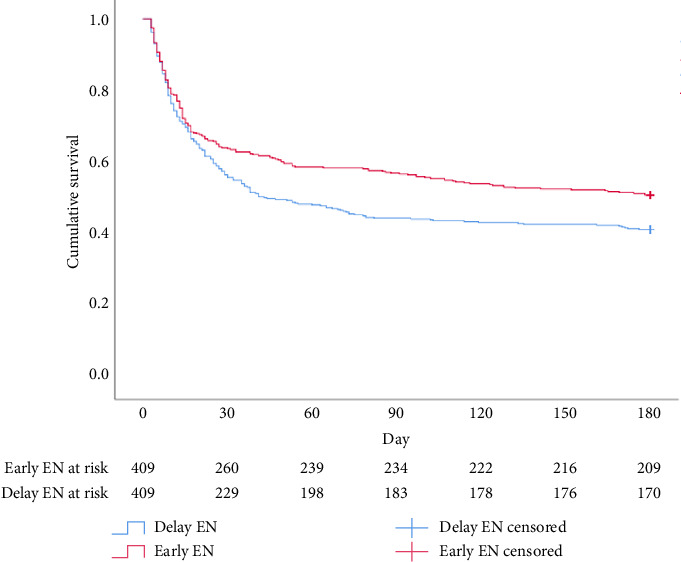
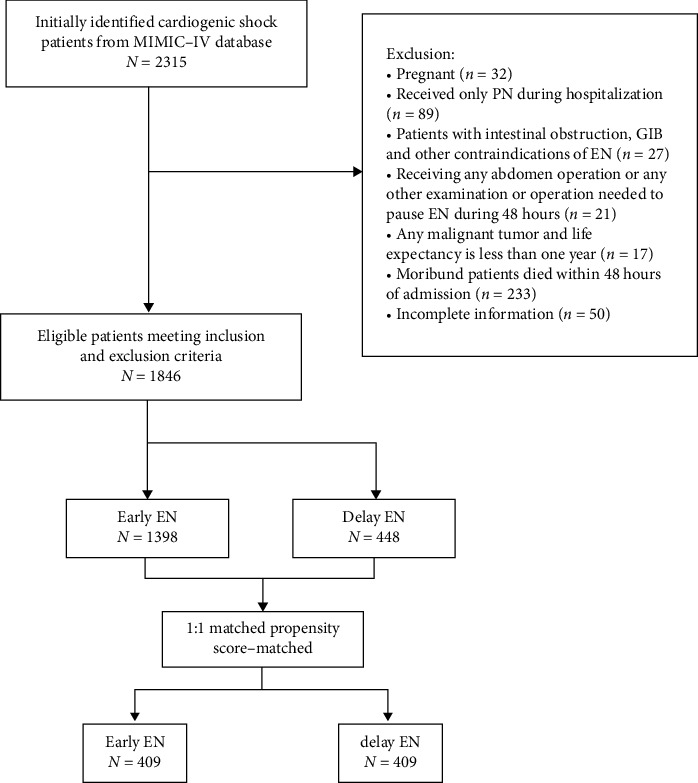
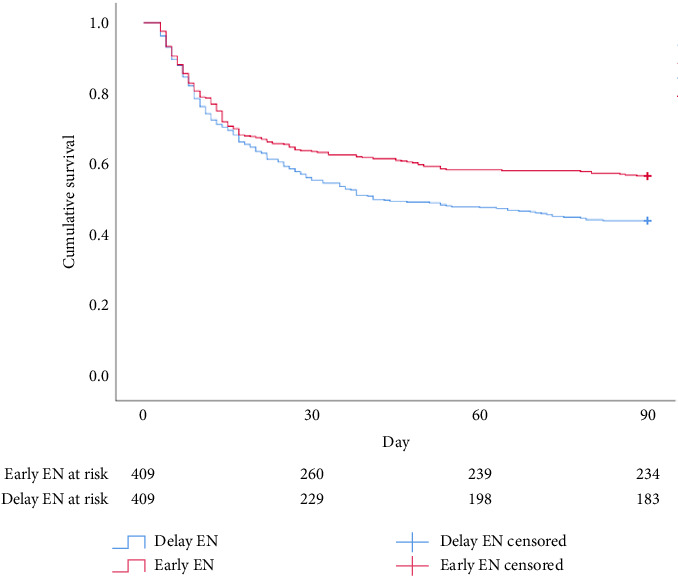
Background and Aim: International guidelines recommend early enteral nutrition (EEN) for critically ill patients. However, evidence supporting the optimal timing of EN in patients diagnosed with cardiogenic shock (CS) is lacking. As such, this study aimed to compare the clinical outcomes and safety of EEN versus delayed EN in patients diagnosed with CS. Methods: This retrospective cohort study was conducted using data from the Medical Information Mart for Intensive Care IV version 2.2 database. Patients who received EN within 2 days of admission were assigned to the EEN group. A 1:1 propensity score-matched (PSM) analysis was performed to control for bias in baseline characteristics and ensure the reliability of the results. To exclude the impact of confounders, an adjusted proportional hazards regression model was used to verify the independence between EEN and survival outcomes. Results: Of 1846 potentially eligible patients, 1398 received EEN and 448 received delayed EN. After 1:1 PSM, 818 patients were assigned to the EEN (n = 409) and delayed EN (n = 409) groups. Regarding cumulative survival, patients with CS receiving EEN experienced better 30-, 90-, and 180-day survival outcomes than the delayed EN group (hazard ratio [HR] 0.803 [95% confidence interval [CI] 0.647-0.998], p=0.045; HR 0.729 [95% CI 0.599-0.889], p=0.001; and HR 0.778 [95% CI 0.644-0.938], p=0.008, respectively). After adjusting for confounders, EEN was found to be independently associated with survival outcomes. Moreover, EEN did not increase the risk(s) for ileus, aspiration pneumonia, or gastrointestinal bleeding. Patients who received delayed EN experienced longer hospital stays than those receiving EEN (17 days [interquartile range [IQR] 10-25] versus 12 days [IQR 7-19 days], respectively; p < 0.001). Conclusion: EEN was not associated with harm, but rather with improved survival outcomes in patients diagnosed with CS. Further studies are required to verify these findings.
期刊介绍:
Emergency Medicine International is a peer-reviewed, Open Access journal that provides a forum for doctors, nurses, paramedics and ambulance staff. The journal publishes original research articles, review articles, and clinical studies related to prehospital care, disaster preparedness and response, acute medical and paediatric emergencies, critical care, sports medicine, wound care, and toxicology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
