Isabelle P Thierry, Steven A Muller, Annette F Baas, Dennis Dooijes, R Laura E van Loon, Angela E Schoemaker, Pim van der Harst, Marish I F J Oerlemans, Hubert F Baars, Rutger J Hassink, Folkert W Asselbergs, J Peter van Tintelen, Anneline S J M Te Riele
{"title":"Yield of family screening for dilated cardiomyopathy: 10-year experience at a multidisciplinary cardiogenetic outpatient clinic.","authors":"Isabelle P Thierry, Steven A Muller, Annette F Baas, Dennis Dooijes, R Laura E van Loon, Angela E Schoemaker, Pim van der Harst, Marish I F J Oerlemans, Hubert F Baars, Rutger J Hassink, Folkert W Asselbergs, J Peter van Tintelen, Anneline S J M Te Riele","doi":"10.1007/s12471-024-01924-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Current family screening approaches in dilated cardiomyopathy (DCM) depend on the presence or absence of a familial genetic variant, in which variant pathogenicity (i.e. benign or pathogenic) classification drives screening recommendations. However, this approach has never been systematically evaluated.</p><p><strong>Methods: </strong>To describe the yield of DCM family screening stratified by variant classification in the Netherlands, we included 358 relatives (mean age ± standard deviation: 44.4 ± 15.9 years at baseline; 52% female; 41% (likely) pathogenic (LP/P) variant carriers from 210 families). Demographics, symptoms and genetic/cardiac test results were obtained. Endpoints were the development of DCM (left ventricular ejection fraction < 50% of non-ischaemic aetiology) or occurrence of major adverse cardiovascular events (MACE) (i.e. heart failure hospitalisation, ventricular arrhythmia or death). Probability of DCM or MACE was assessed with the Kaplan-Meier method.</p><p><strong>Results: </strong>DCM was present in 32 relatives (9%) (25/32 (78%) with LP/P variant) at baseline and in an additional 10/97 relatives (10%) (9/10 (90%) with LP/P variant) who were re-evaluated during a median follow-up time of 5.0 years (interquartile range: 3.2-7.4). Of the 128 relatives without the familial LP/P variant, none developed DCM. MACE was experienced by 5 relatives (1%) (4/5 (80%) with LP/P variant), all of whom had DCM at the time of the event.</p><p><strong>Conclusion: </strong>The yield of DCM family screening was ~10% at baseline and another ~10% during 5‑year follow-up. Relatives without the familial LP/P variant could be safely discharged. These results reinforce the use of a genetics-first screening approach in relatives from families with an LP/P variant. This will lower the burden on resources in Dutch hospitals and help allocate resources to those who are most likely to benefit.</p>","PeriodicalId":18952,"journal":{"name":"Netherlands Heart Journal","volume":" ","pages":"46-54"},"PeriodicalIF":2.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11757811/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Netherlands Heart Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12471-024-01924-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
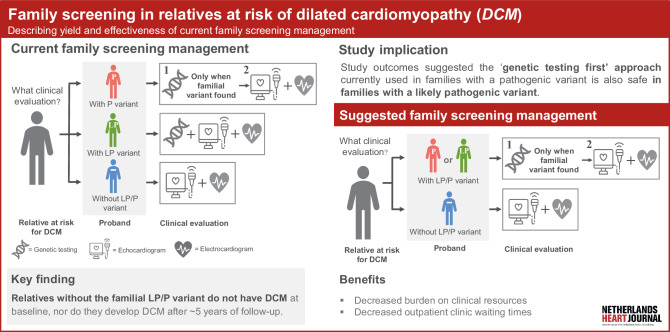
Introduction: Current family screening approaches in dilated cardiomyopathy (DCM) depend on the presence or absence of a familial genetic variant, in which variant pathogenicity (i.e. benign or pathogenic) classification drives screening recommendations. However, this approach has never been systematically evaluated.
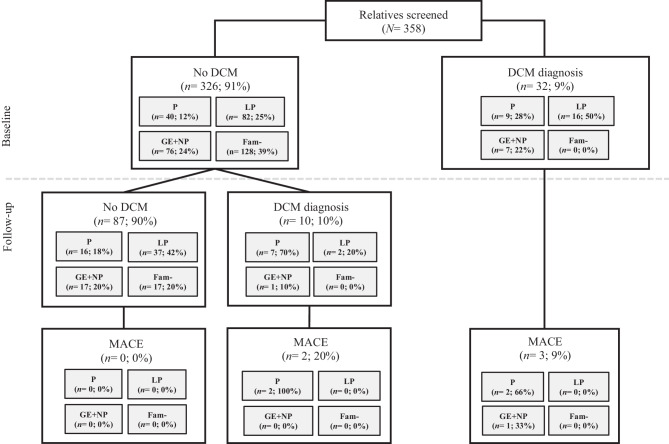
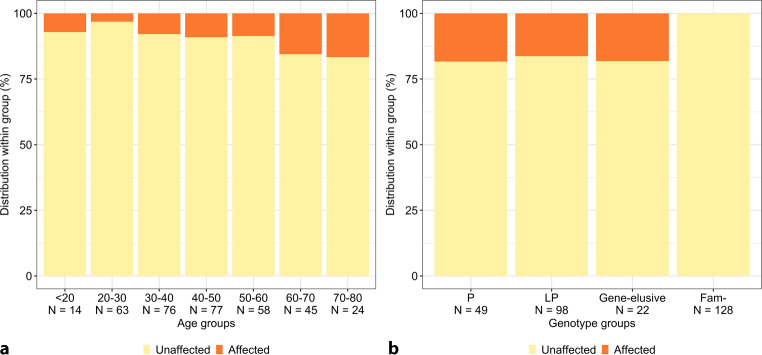
Methods: To describe the yield of DCM family screening stratified by variant classification in the Netherlands, we included 358 relatives (mean age ± standard deviation: 44.4 ± 15.9 years at baseline; 52% female; 41% (likely) pathogenic (LP/P) variant carriers from 210 families). Demographics, symptoms and genetic/cardiac test results were obtained. Endpoints were the development of DCM (left ventricular ejection fraction < 50% of non-ischaemic aetiology) or occurrence of major adverse cardiovascular events (MACE) (i.e. heart failure hospitalisation, ventricular arrhythmia or death). Probability of DCM or MACE was assessed with the Kaplan-Meier method.
Results: DCM was present in 32 relatives (9%) (25/32 (78%) with LP/P variant) at baseline and in an additional 10/97 relatives (10%) (9/10 (90%) with LP/P variant) who were re-evaluated during a median follow-up time of 5.0 years (interquartile range: 3.2-7.4). Of the 128 relatives without the familial LP/P variant, none developed DCM. MACE was experienced by 5 relatives (1%) (4/5 (80%) with LP/P variant), all of whom had DCM at the time of the event.
Conclusion: The yield of DCM family screening was ~10% at baseline and another ~10% during 5‑year follow-up. Relatives without the familial LP/P variant could be safely discharged. These results reinforce the use of a genetics-first screening approach in relatives from families with an LP/P variant. This will lower the burden on resources in Dutch hospitals and help allocate resources to those who are most likely to benefit.
期刊介绍:
The scope of the Netherlands Heart Journal is to contribute to the national and international literature by publishing scientific papers in the field of cardiovascular medicine. It also provides a platform for Continuing Medical Education for cardiologists and those in training for the speciality of cardiology in the Netherlands.
The Netherlands Heart Journal is made available to cardiologists, cardiologists in training, cardiopulmonary surgeons, cardiopulmonary surgeons in training, internists and paediatric cardiologists. The journal is the official journal of the Netherlands Society of Cardiology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
