Lin Cheng, Sheng Xu, Yu-Feng Wang, Sheng-Wei Li, Bin Li, Xiao-Guang Li
{"title":"Circulating Tumor DNA Detection for Recurrence Monitoring of Stage I Non-Small Cell Lung Cancer Treated With Microwave Ablation.","authors":"Lin Cheng, Sheng Xu, Yu-Feng Wang, Sheng-Wei Li, Bin Li, Xiao-Guang Li","doi":"10.1111/1759-7714.15534","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>As microwave ablation continues to be used in patients with inoperable stage I non-small cell lung cancer (NSCLC), it is particularly important to monitor efficacy. Whether plasma ctDNA detection can predict its efficacy should be illustrated.</p><p><strong>Methods: </strong>We recruited 43 patients with inoperative stage I NSCLC, all of whom underwent biopsy-synchronous microwave ablation (MWA). Peripheral blood samples were collected at baseline (n = 43), within 1 h post-MWA (n = 28), and at the landmark time point (n = 26) for MRD detection. Clinical outcomes were analyzed using Kaplan-Meier survival analysis.</p><p><strong>Results: </strong>Patients with undetectable ctDNA at baseline (p = 0.042) and within 1 h after MWA (p = 0.023) had better clinical outcomes. In particular, patients with undetectable ctDNA at the 1-h post-MWA time point did not experience recurrence. Detection of ctDNA at the landmark time point is considered an independent risk factor for prognosis and is strongly correlated with clinical outcomes (p = 0.001), the median time to recurrence indicated by ctDNA was 4.9 months earlier compared to imaging. The clinical outcomes of patients with ctDNA clearance were similar to those with no ctDNA (p = 0.570). Risk stratification indicated that patients with persistent ctDNA had worse clinical outcomes compared to those who never had detectable ctDNA (p = 0.004).</p><p><strong>Conclusion: </strong>Our findings suggest that ctDNA monitoring can assist in predicting clinical outcomes in stage I NSCLC treated with microwave ablation. Patients with undetectable ctDNA within 1 h after MWA are determined to be clinically cured. Risk stratification based on ctDNA test results helps to differentiate high-risk patients.</p>","PeriodicalId":23338,"journal":{"name":"Thoracic Cancer","volume":"16 2","pages":"e15534"},"PeriodicalIF":2.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11742128/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/1759-7714.15534","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: As microwave ablation continues to be used in patients with inoperable stage I non-small cell lung cancer (NSCLC), it is particularly important to monitor efficacy. Whether plasma ctDNA detection can predict its efficacy should be illustrated.
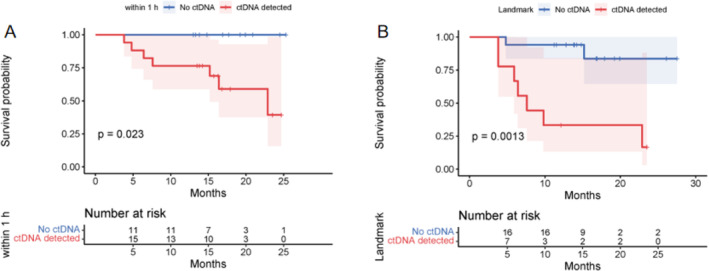
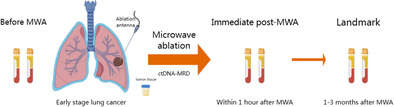
Methods: We recruited 43 patients with inoperative stage I NSCLC, all of whom underwent biopsy-synchronous microwave ablation (MWA). Peripheral blood samples were collected at baseline (n = 43), within 1 h post-MWA (n = 28), and at the landmark time point (n = 26) for MRD detection. Clinical outcomes were analyzed using Kaplan-Meier survival analysis.
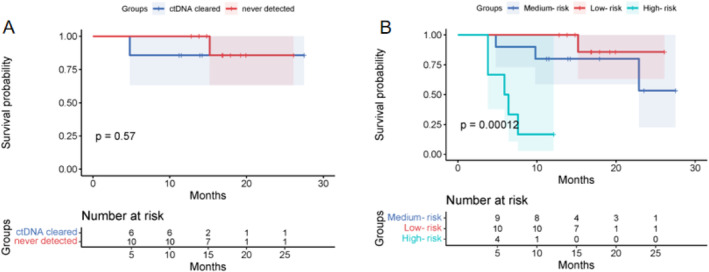
Results: Patients with undetectable ctDNA at baseline (p = 0.042) and within 1 h after MWA (p = 0.023) had better clinical outcomes. In particular, patients with undetectable ctDNA at the 1-h post-MWA time point did not experience recurrence. Detection of ctDNA at the landmark time point is considered an independent risk factor for prognosis and is strongly correlated with clinical outcomes (p = 0.001), the median time to recurrence indicated by ctDNA was 4.9 months earlier compared to imaging. The clinical outcomes of patients with ctDNA clearance were similar to those with no ctDNA (p = 0.570). Risk stratification indicated that patients with persistent ctDNA had worse clinical outcomes compared to those who never had detectable ctDNA (p = 0.004).
Conclusion: Our findings suggest that ctDNA monitoring can assist in predicting clinical outcomes in stage I NSCLC treated with microwave ablation. Patients with undetectable ctDNA within 1 h after MWA are determined to be clinically cured. Risk stratification based on ctDNA test results helps to differentiate high-risk patients.
期刊介绍:
Thoracic Cancer aims to facilitate international collaboration and exchange of comprehensive and cutting-edge information on basic, translational, and applied clinical research in lung cancer, esophageal cancer, mediastinal cancer, breast cancer and other thoracic malignancies. Prevention, treatment and research relevant to Asia-Pacific is a focus area, but submissions from all regions are welcomed. The editors encourage contributions relevant to prevention, general thoracic surgery, medical oncology, radiology, radiation medicine, pathology, basic cancer research, as well as epidemiological and translational studies in thoracic cancer. Thoracic Cancer is the official publication of the Chinese Society of Lung Cancer, International Chinese Society of Thoracic Surgery and is endorsed by the Korean Association for the Study of Lung Cancer and the Hong Kong Cancer Therapy Society.
The Journal publishes a range of article types including: Editorials, Invited Reviews, Mini Reviews, Original Articles, Clinical Guidelines, Technological Notes, Imaging in thoracic cancer, Meeting Reports, Case Reports, Letters to the Editor, Commentaries, and Brief Reports.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
