{"title":"Glycoprotein 350-targeted chimeric antigen receptor T-cell therapy for nonneoplastic chronic active Epstein-Barr virus infection: a case report.","authors":"Yandi Liu, Jiaoyang Cai, Tianyi Wang, Jing Wang, Yanjing Tang, Xinyu Wan, Wenjie Li, Benshang Li, Qing Cao","doi":"10.21037/tp-24-292","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic active Epstein-Barr virus (CAEBV) infection is a rare disease in which the Epstein-Barr virus (EBV) persists and replicates, causing chronic symptoms and fatal complications. The treatment of CAEBV is still evolving. Our case report showed a new therapy for CAEBV.</p><p><strong>Case description: </strong>A 14-year-old boy presented with a 10-month history of recurrent diarrhea, intermittent fever, abdominal pain, distension, dizziness, and fatigue. Physical examination findings included severe malnutrition and hepatosplenomegaly. The local hospital's test results showed that the load of EBV DNA in peripheral blood was 5.99×10<sup>6</sup> copies/mL. Despite treatment with acyclovir, chemotherapy, and supportive care, the symptoms persisted. We determined the lymphocyte subtypes of EBV infection by fluorescence quantitative polymerase chain reaction and the expression of EBV envelope glycoprotein 350 (gp350) in peripheral blood lymphocytes. EBV not only infects B cells but also T and NK cells. According to the clinical manifestations, elevated EBV DNA levels, and positive EBV-encoded small RNA (EBER) status, the patient was diagnosed with CAEBV infection. The patient received a conditioning regimen of fludarabine and cyclophosphamide and an intravenous infusion of gp350-targeted chimeric antigen receptor T (CAR T) cells. After infusion, the patient developed grade I cytokine release syndrome (CRS) and was discharged 10 days later. During the follow-up, the EBV-DNA count remained undetectable.</p><p><strong>Conclusions: </strong>Our case report showed that CAR T-cell therapy is relatively safe and effective for treating CAEBV in children, with milder CRS compared to that in malignant tumors. However, a greater number of cases are needed to further evaluate the efficacy and safety.</p>","PeriodicalId":23294,"journal":{"name":"Translational pediatrics","volume":"13 12","pages":"2305-2310"},"PeriodicalIF":1.7000,"publicationDate":"2024-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732635/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tp-24-292","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chronic active Epstein-Barr virus (CAEBV) infection is a rare disease in which the Epstein-Barr virus (EBV) persists and replicates, causing chronic symptoms and fatal complications. The treatment of CAEBV is still evolving. Our case report showed a new therapy for CAEBV.
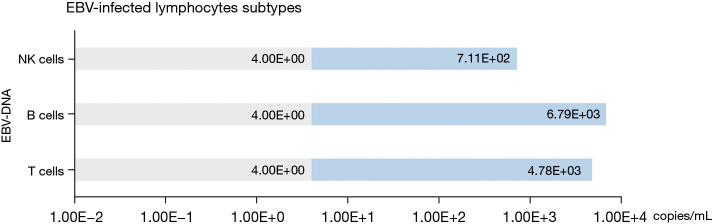
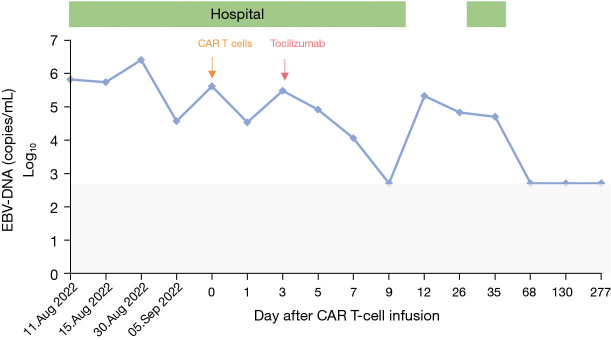
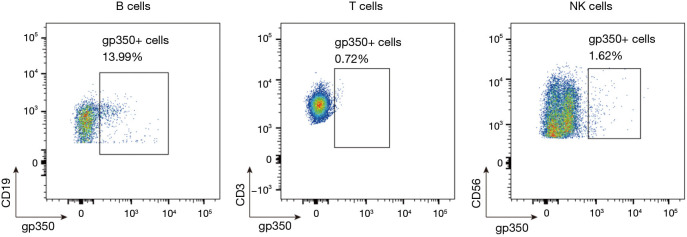
Case description: A 14-year-old boy presented with a 10-month history of recurrent diarrhea, intermittent fever, abdominal pain, distension, dizziness, and fatigue. Physical examination findings included severe malnutrition and hepatosplenomegaly. The local hospital's test results showed that the load of EBV DNA in peripheral blood was 5.99×106 copies/mL. Despite treatment with acyclovir, chemotherapy, and supportive care, the symptoms persisted. We determined the lymphocyte subtypes of EBV infection by fluorescence quantitative polymerase chain reaction and the expression of EBV envelope glycoprotein 350 (gp350) in peripheral blood lymphocytes. EBV not only infects B cells but also T and NK cells. According to the clinical manifestations, elevated EBV DNA levels, and positive EBV-encoded small RNA (EBER) status, the patient was diagnosed with CAEBV infection. The patient received a conditioning regimen of fludarabine and cyclophosphamide and an intravenous infusion of gp350-targeted chimeric antigen receptor T (CAR T) cells. After infusion, the patient developed grade I cytokine release syndrome (CRS) and was discharged 10 days later. During the follow-up, the EBV-DNA count remained undetectable.
Conclusions: Our case report showed that CAR T-cell therapy is relatively safe and effective for treating CAEBV in children, with milder CRS compared to that in malignant tumors. However, a greater number of cases are needed to further evaluate the efficacy and safety.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
