Exploring the influence of medical staffing and birth volume on observed-to-expected cesarean deliveries: a panel data analysis of integrated obstetric and gynecological departments in Germany.
Arno Stöcker, Holger Pfaff, Nadine Scholten, Ludwig Kuntz
{"title":"Exploring the influence of medical staffing and birth volume on observed-to-expected cesarean deliveries: a panel data analysis of integrated obstetric and gynecological departments in Germany.","authors":"Arno Stöcker, Holger Pfaff, Nadine Scholten, Ludwig Kuntz","doi":"10.1007/s10198-024-01749-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cesarean deliveries account for approximately one-third of all births in Germany, prompting ongoing discussions on cesarean section rates and their connection to medical staffing and birth volume. In Germany, the majority of departments integrate obstetric and gynecological care within a single department.</p><p><strong>Methods: </strong>The analysis utilized quality reports from German hospitals spanning 2015 to 2019. The outcome variable was the annual risk-adjusted cesarean section ratio-a metric comparing expected to observed cesarean sections. Explanatory variables included annual counts of physicians, midwives, and births. To account for case number-related staffing variations, full-time equivalent midwife and physician staff positions were normalized by the number of deliveries. Uni- and multivariate panel models were applied, complemented by multiple instrument variable analyses, including two-stage least square and generalized method of moments models.</p><p><strong>Results: </strong>Incorporating data from 509 integrated obstetric departments and 2089 observations, representing 2,335,839 deliveries with 720,795 cesarean sections (over 60% of all inpatient births in Germany), multivariate model with fixed effects revealed a statistically significant positive association between the number of physicians per birth and the risk-adjusted cesarean section ratio (0.004, p = 0.004). Two-stage least square instrument variable analysis (0.020, p < 0.001) and a system GMM estimator models (0.004, p < 0.001) validated these results, providing compelling evidence for a causal relationship.</p><p><strong>Conclusion: </strong>The study established a robust connection between the number of physicians per birth and the risk-adjusted cesarean section ratio in integrated obstetric and gynecological departments in Germany. While the cause of the effect remains unclear, one possible explanation is a lack of specialization within these departments due to the combined provision of both obstetric and gynecological care.</p>","PeriodicalId":51416,"journal":{"name":"European Journal of Health Economics","volume":" ","pages":"987-1022"},"PeriodicalIF":3.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12310771/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Health Economics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10198-024-01749-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Cesarean deliveries account for approximately one-third of all births in Germany, prompting ongoing discussions on cesarean section rates and their connection to medical staffing and birth volume. In Germany, the majority of departments integrate obstetric and gynecological care within a single department.
Methods: The analysis utilized quality reports from German hospitals spanning 2015 to 2019. The outcome variable was the annual risk-adjusted cesarean section ratio-a metric comparing expected to observed cesarean sections. Explanatory variables included annual counts of physicians, midwives, and births. To account for case number-related staffing variations, full-time equivalent midwife and physician staff positions were normalized by the number of deliveries. Uni- and multivariate panel models were applied, complemented by multiple instrument variable analyses, including two-stage least square and generalized method of moments models.
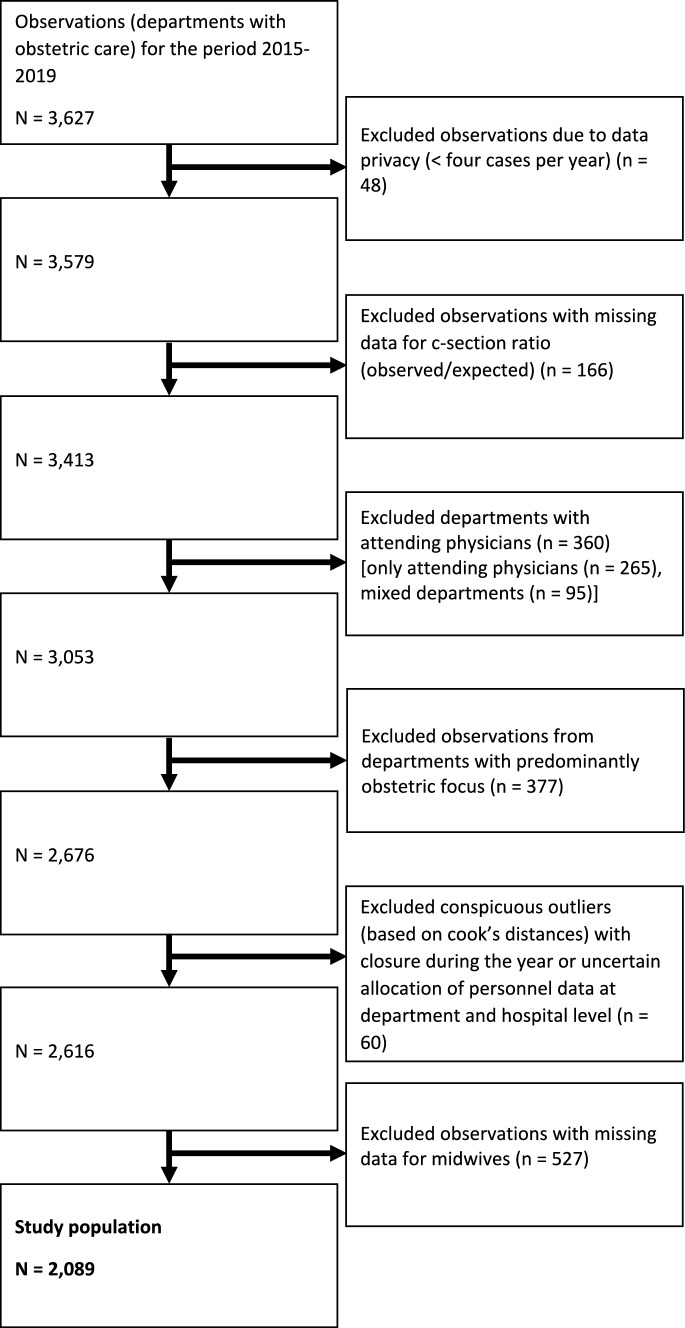
Results: Incorporating data from 509 integrated obstetric departments and 2089 observations, representing 2,335,839 deliveries with 720,795 cesarean sections (over 60% of all inpatient births in Germany), multivariate model with fixed effects revealed a statistically significant positive association between the number of physicians per birth and the risk-adjusted cesarean section ratio (0.004, p = 0.004). Two-stage least square instrument variable analysis (0.020, p < 0.001) and a system GMM estimator models (0.004, p < 0.001) validated these results, providing compelling evidence for a causal relationship.
Conclusion: The study established a robust connection between the number of physicians per birth and the risk-adjusted cesarean section ratio in integrated obstetric and gynecological departments in Germany. While the cause of the effect remains unclear, one possible explanation is a lack of specialization within these departments due to the combined provision of both obstetric and gynecological care.
期刊介绍:
The European Journal of Health Economics is a journal of Health Economics and associated disciplines. The growing demand for health economics and the introduction of new guidelines in various European countries were the motivation to generate a highly scientific and at the same time practice oriented journal considering the requirements of various health care systems in Europe. The international scientific board of opinion leaders guarantees high-quality, peer-reviewed publications as well as articles for pragmatic approaches in the field of health economics. We intend to cover all aspects of health economics:
• Basics of health economic approaches and methods
• Pharmacoeconomics
• Health Care Systems
• Pricing and Reimbursement Systems
• Quality-of-Life-Studies The editors reserve the right to reject manuscripts that do not comply with the above-mentioned requirements. The author will be held responsible for false statements or for failure to fulfill the above-mentioned requirements.
Officially cited as: Eur J Health Econ




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
