Ragini Kondetimmanahalli, Jane Lynch, Gary Francis, Heather Gardner, Radhika Pillai
{"title":"Pseudohypoparathyroidism type 1A presenting as short stature and congenital hypothyroidism.","authors":"Ragini Kondetimmanahalli, Jane Lynch, Gary Francis, Heather Gardner, Radhika Pillai","doi":"10.1530/EDM-24-0097","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>Short stature is a common complaint among pediatric visits and the differential diagnosis is extensive. Although some variations in growth are normal, deviation from normal growth is often the first symptom of chronic disease in children. This is true for hormone abnormalities including growth hormone deficiency, hypothyroidism and glucocorticoid excess. However, reduced growth velocity can also occur as the first sign of chronic anemia, malnutrition, deprivation (psychosocial dwarfism), chromosomal abnormalities, genetic syndromes and inflammatory bowel diseases. For the primary care provider, simple measures of standing height, sitting height, arm span, weight, body mass index (BMI) and bone age (BA) will lead to the correct diagnosis in most short children. Screening laboratory studies for endocrine disorders, a skeletal survey if skeletal disproportion is evident, a karyotype or microarray (microarray favored if developmental delay is also present) and genetic testing for monogenic disorders will lead to a specific diagnosis in an additional subset of short children. This case presented a diagnostic dilemma that spanned all these possibilities and served as a focal point for the review of normal growth and growth abnormalities.</p><p><strong>Learning points: </strong>Variations in growth can be normal variants (constitutional delay of growth and puberty or familial short stature) but deviation from normal growth can also be the first sign of an underlying pathological process. Measures of standing height, sitting height, arm span, weight, body mass index (BMI) and bone age (BA) will lead to the correct diagnosis in 50-80% of short children. Screening laboratory studies for endocrine disorders, a skeletal survey if skeletal disproportion is evident, a karyotype or microarray (microarray is favored if developmental delay is also present) and genetic testing will lead to a specific diagnosis in another 35% of short children. Pseudohypoparathyroidism (PHP) type 1A is due to a mutation in the alpha subunit of the stimulatory G protein of the guanine nucleotide-binding protein gene. Multiple hormone resistance often affects thyroid-stimulating hormone and, when presenting in the newborn period, can be misdiagnosed as common forms of congenital hypothyroidism. Molecular testing is an important component of confirming the diagnosis and PHP subtype, which can help guide management.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":"2025 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11811821/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-24-0097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"Print","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
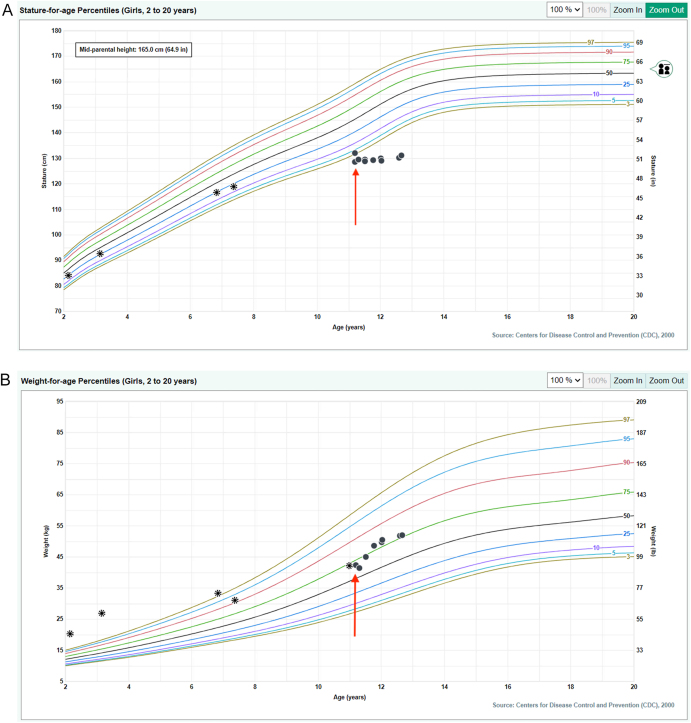
Summary: Short stature is a common complaint among pediatric visits and the differential diagnosis is extensive. Although some variations in growth are normal, deviation from normal growth is often the first symptom of chronic disease in children. This is true for hormone abnormalities including growth hormone deficiency, hypothyroidism and glucocorticoid excess. However, reduced growth velocity can also occur as the first sign of chronic anemia, malnutrition, deprivation (psychosocial dwarfism), chromosomal abnormalities, genetic syndromes and inflammatory bowel diseases. For the primary care provider, simple measures of standing height, sitting height, arm span, weight, body mass index (BMI) and bone age (BA) will lead to the correct diagnosis in most short children. Screening laboratory studies for endocrine disorders, a skeletal survey if skeletal disproportion is evident, a karyotype or microarray (microarray favored if developmental delay is also present) and genetic testing for monogenic disorders will lead to a specific diagnosis in an additional subset of short children. This case presented a diagnostic dilemma that spanned all these possibilities and served as a focal point for the review of normal growth and growth abnormalities.
Learning points: Variations in growth can be normal variants (constitutional delay of growth and puberty or familial short stature) but deviation from normal growth can also be the first sign of an underlying pathological process. Measures of standing height, sitting height, arm span, weight, body mass index (BMI) and bone age (BA) will lead to the correct diagnosis in 50-80% of short children. Screening laboratory studies for endocrine disorders, a skeletal survey if skeletal disproportion is evident, a karyotype or microarray (microarray is favored if developmental delay is also present) and genetic testing will lead to a specific diagnosis in another 35% of short children. Pseudohypoparathyroidism (PHP) type 1A is due to a mutation in the alpha subunit of the stimulatory G protein of the guanine nucleotide-binding protein gene. Multiple hormone resistance often affects thyroid-stimulating hormone and, when presenting in the newborn period, can be misdiagnosed as common forms of congenital hypothyroidism. Molecular testing is an important component of confirming the diagnosis and PHP subtype, which can help guide management.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
