Divya B. Dasani , Maria Isabel Fiel , Camila C. Simoes , Adam S. Morgenthau , Thomas D. Schiano
{"title":"The Varying Histology of Hepatic Sarcoidosis and the Relation of Bile Duct Damage and Loss to the Presence of Portal Hypertension and Cirrhosis","authors":"Divya B. Dasani , Maria Isabel Fiel , Camila C. Simoes , Adam S. Morgenthau , Thomas D. Schiano","doi":"10.1016/j.gastha.2024.10.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and Aims</h3><div>Sarcoidosis is a multisystem disorder characterized by nonnecrotizing granulomas. Studies suggest 20%–70% of patients with sarcoidosis have abnormal liver chemistries or abdominal imaging. Hepatic sarcoidosis may be complicated by portal hypertension (portal HTN) with or without cirrhosis. Few studies have reviewed the liver histopathology of sarcoidosis.</div></div><div><h3>Methods</h3><div>Searching the pathology database using the terms “sarcoidosis” and “liver,” patients were identified and cross-referenced to patients in the Sarcoidosis Clinic. Patients met the diagnostic criteria for sarcoidosis. Those with isolated granulomatous hepatitis were excluded. Demographics, abdominal imaging, biochemistries, and detailed histological features were cataloged.</div></div><div><h3>Results</h3><div>Patients were separated into 2 groups: those with portal HTN with or without cirrhosis (pHTN+) and those without portal HTN (pHTN-). Fifty-three patients had biopsies available for review (pHTN+, n = 33; pHTN-, n = 20). The groups did not differ in the location, type, or number of granulomas. The pHTN + group had more bile duct damage (<em>P</em> = .025) and loss (<em>P</em> = .019). Patients in the pHTN + group also had biliary cirrhosis, nodular regenerative hyperplasia, or outflow obstruction.</div></div><div><h3>Conclusion</h3><div>There are several causes for portal HTN in sarcoidosis. Thus, liver biopsy is essential in its evaluation. Bile duct damage and loss are associated with the presence of portal HTN and cirrhosis. Biliary abnormalities may occur independently of granulomatous inflammation, and can thus identify a subset of patients at risk for progressive liver disease.</div></div>","PeriodicalId":73130,"journal":{"name":"Gastro hep advances","volume":"4 2","pages":"Article 100561"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11757786/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastro hep advances","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772572324001560","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and Aims
Sarcoidosis is a multisystem disorder characterized by nonnecrotizing granulomas. Studies suggest 20%–70% of patients with sarcoidosis have abnormal liver chemistries or abdominal imaging. Hepatic sarcoidosis may be complicated by portal hypertension (portal HTN) with or without cirrhosis. Few studies have reviewed the liver histopathology of sarcoidosis.
Methods
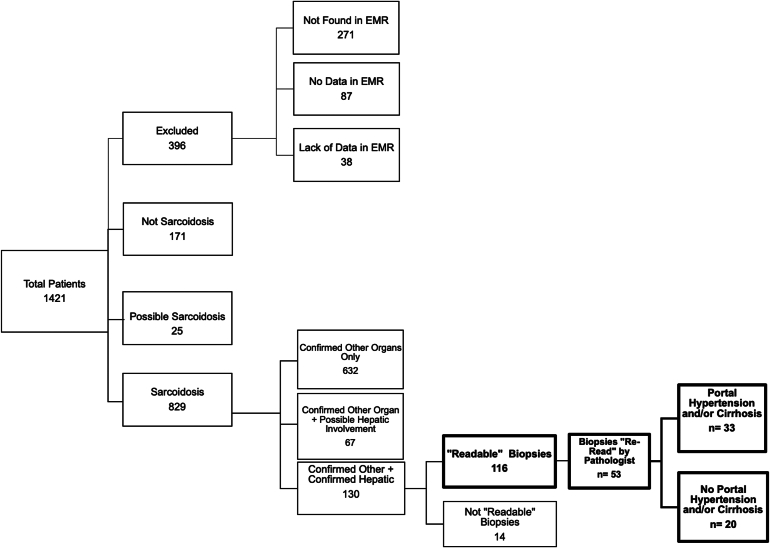
Searching the pathology database using the terms “sarcoidosis” and “liver,” patients were identified and cross-referenced to patients in the Sarcoidosis Clinic. Patients met the diagnostic criteria for sarcoidosis. Those with isolated granulomatous hepatitis were excluded. Demographics, abdominal imaging, biochemistries, and detailed histological features were cataloged.
Results
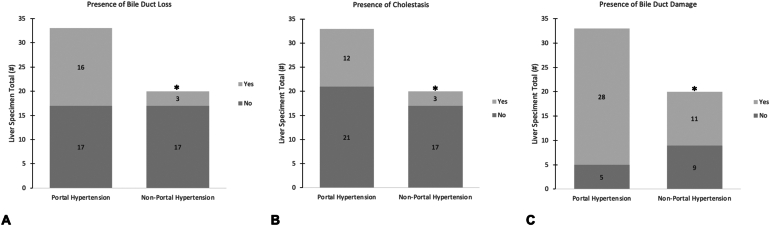
Patients were separated into 2 groups: those with portal HTN with or without cirrhosis (pHTN+) and those without portal HTN (pHTN-). Fifty-three patients had biopsies available for review (pHTN+, n = 33; pHTN-, n = 20). The groups did not differ in the location, type, or number of granulomas. The pHTN + group had more bile duct damage (P = .025) and loss (P = .019). Patients in the pHTN + group also had biliary cirrhosis, nodular regenerative hyperplasia, or outflow obstruction.
Conclusion
There are several causes for portal HTN in sarcoidosis. Thus, liver biopsy is essential in its evaluation. Bile duct damage and loss are associated with the presence of portal HTN and cirrhosis. Biliary abnormalities may occur independently of granulomatous inflammation, and can thus identify a subset of patients at risk for progressive liver disease.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
