A Nonrandomized Pilot Study to Investigate the Acceptability and Feasibility of LivR Well: A Multifaceted 28-Day Home-Based Liver Optimization Program for Acute-on-Chronic Liver Failure
Natalie L.Y. Ngu , Edward Saxby , Thomas Worland , Patricia Anderson , Lisa Stothers , Jo Hunter , Alexander T. Elford , Phil Ha , Imogen Hartley , Andrew Roberts , Dean Seah , George Tambakis , Declan Connoley , Anita Figredo , Dilip Ratnam , Danny Liew , Benjamin Rogers , William Sievert , Sally Bell , Suong Le
{"title":"A Nonrandomized Pilot Study to Investigate the Acceptability and Feasibility of LivR Well: A Multifaceted 28-Day Home-Based Liver Optimization Program for Acute-on-Chronic Liver Failure","authors":"Natalie L.Y. Ngu , Edward Saxby , Thomas Worland , Patricia Anderson , Lisa Stothers , Jo Hunter , Alexander T. Elford , Phil Ha , Imogen Hartley , Andrew Roberts , Dean Seah , George Tambakis , Declan Connoley , Anita Figredo , Dilip Ratnam , Danny Liew , Benjamin Rogers , William Sievert , Sally Bell , Suong Le","doi":"10.1016/j.gastha.2024.10.007","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and Aims</h3><div>Acute-on-chronic liver failure (ACLF) has a 22%–74% 28-day mortality rate and 30%–40% 30-day readmission rate. We investigated the acceptability and feasibility of a multimodal community intervention for ACLF.</div></div><div><h3>Methods</h3><div>A single-arm nonrandomized pilot study of consecutive participants with ACLF was conducted in a tertiary health service. Participants received weekly medical and nursing reviews, dietetics, physiotherapy, pharmacy, social work, addiction medicine, and neuropsychiatry, where indicated. A digital platform included remote weight monitoring and online surveys. The primary outcome was acceptability/feasibility. Secondary outcomes included safety, mortality, readmission, liver disease severity, and costs.</div></div><div><h3>Results</h3><div>Fifty-nine patients were enrolled with median age 51 years (interquartile range (IQR): 45–59); majority alcohol etiology (74%),and median Model for End-Stage Liver Disease Sodium score 16 (IQR: 12–21). LivR Well was acceptable with low attrition (8 of 59), adherence to the program including home visits (mean 8.4 ± 4.2) and consultations (mean 2.4 ± 1.5) per patient. This was supported by positive feedback and themes identified through a qualitative subanalysis. Feasibility was demonstrated by recruitment rate of 4.94 patients/month and 86% completion. Mortality was lower than expected at 3%, 30-day readmission rate was 15%, and median Model for End-Stage Liver Disease Sodium score reduced to 15 (<em>P</em> = .01). Median 6-month costs reduced from $30,454 (IQR: $21,953–$65,657) to $17,657 ($4249–$42,876) (<em>P</em> = .009). The total 6-month health-care cost was $1,868,859 (95% confidence interval 1,081,821–2,655,897) compared to $2,518,227 (95% confidence interval 1,959,610–3,076,844).</div></div><div><h3>Conclusion</h3><div>LivR Well was acceptable, feasible, and safe with low short-term mortality and readmission rates. Health-care costs were reduced by 26% driven by a 40% reduction in 30-day readmission. Further evaluation includes a randomized controlled trial of LivR Well compared to standard care.</div></div>","PeriodicalId":73130,"journal":{"name":"Gastro hep advances","volume":"4 2","pages":"Article 100567"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11773469/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastro hep advances","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772572324001626","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/18 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and Aims
Acute-on-chronic liver failure (ACLF) has a 22%–74% 28-day mortality rate and 30%–40% 30-day readmission rate. We investigated the acceptability and feasibility of a multimodal community intervention for ACLF.
Methods
A single-arm nonrandomized pilot study of consecutive participants with ACLF was conducted in a tertiary health service. Participants received weekly medical and nursing reviews, dietetics, physiotherapy, pharmacy, social work, addiction medicine, and neuropsychiatry, where indicated. A digital platform included remote weight monitoring and online surveys. The primary outcome was acceptability/feasibility. Secondary outcomes included safety, mortality, readmission, liver disease severity, and costs.
Results
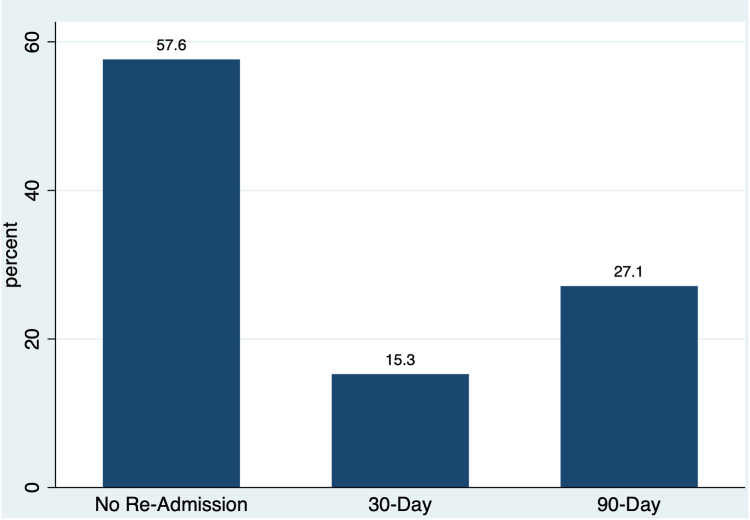
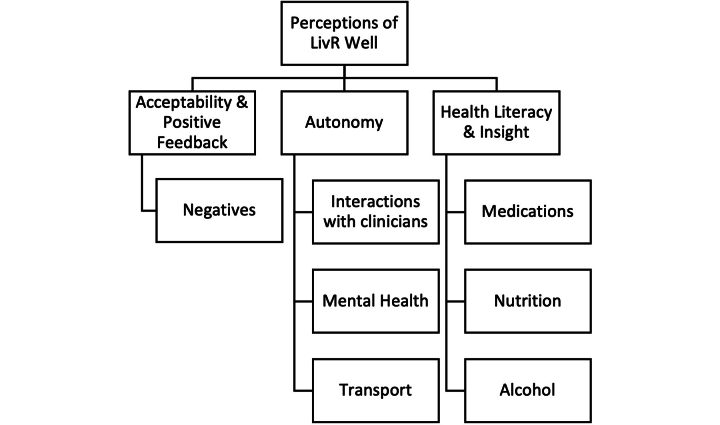
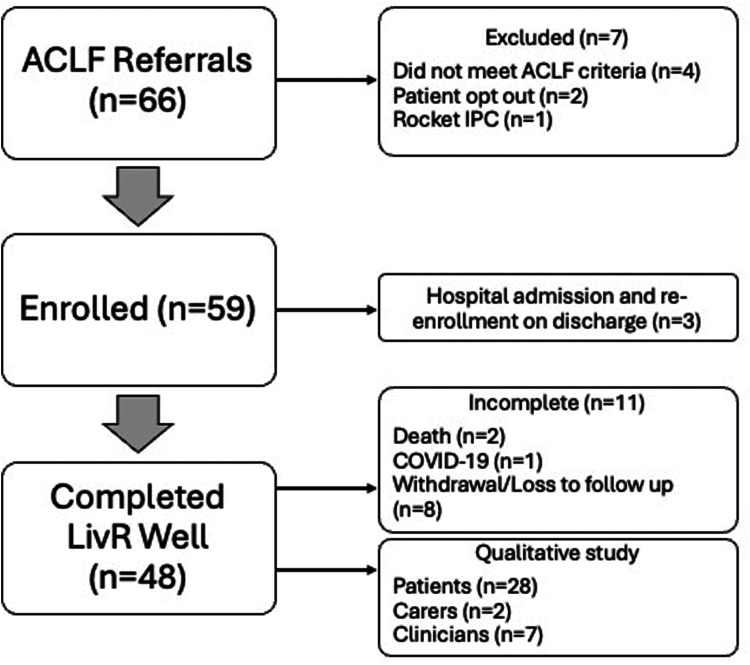
Fifty-nine patients were enrolled with median age 51 years (interquartile range (IQR): 45–59); majority alcohol etiology (74%),and median Model for End-Stage Liver Disease Sodium score 16 (IQR: 12–21). LivR Well was acceptable with low attrition (8 of 59), adherence to the program including home visits (mean 8.4 ± 4.2) and consultations (mean 2.4 ± 1.5) per patient. This was supported by positive feedback and themes identified through a qualitative subanalysis. Feasibility was demonstrated by recruitment rate of 4.94 patients/month and 86% completion. Mortality was lower than expected at 3%, 30-day readmission rate was 15%, and median Model for End-Stage Liver Disease Sodium score reduced to 15 (P = .01). Median 6-month costs reduced from $30,454 (IQR: $21,953–$65,657) to $17,657 ($4249–$42,876) (P = .009). The total 6-month health-care cost was $1,868,859 (95% confidence interval 1,081,821–2,655,897) compared to $2,518,227 (95% confidence interval 1,959,610–3,076,844).
Conclusion
LivR Well was acceptable, feasible, and safe with low short-term mortality and readmission rates. Health-care costs were reduced by 26% driven by a 40% reduction in 30-day readmission. Further evaluation includes a randomized controlled trial of LivR Well compared to standard care.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
