{"title":"Finding the Culprit: Cushing Syndrome Secondary to Lung Carcinoid Tumor","authors":"Richard Vaca MD , Nirali A. Shah MD","doi":"10.1016/j.aace.2024.09.002","DOIUrl":null,"url":null,"abstract":"<div><h3>Background/Objective</h3><div>Cushing syndrome resulting from ectopic adrenocorticotropic hormone (ACTH) secretion (EAS) is a rare condition, and its occurrence in adolescents is even more uncommon, representing <1% of cases. We describe a case of EAS from a lung carcinoid tumor leading to Cushing syndrome in a young woman, which was successfully treated with excision of the tumor.</div></div><div><h3>Case Report</h3><div>An 18-year-old woman presented with mood disturbances, weight gain, and fatigue for 6 months. Workup revealed high levels of urinary free cortisol (>900 μg/dL; normal range, <45 μg/dL) and midnight salivary cortisol (0.755 μg/dL; normal range, <0.09 μg/dL). The ACTH and cortisol levels remained elevated after a low-dose dexamethasone suppression test. Magnetic resonance imaging of the pituitary gland did not reveal any adenoma and inferior petrosal sinus sampling showed no central-to-peripheral gradient. A diagnosis of EAS was made. Subsequent body imaging noted a 1-cm lung nodule. Due to symptoms of severe hypercortisolism including hypokalemia and worsening mood changes, the patient was started on metyrapone as a bridge to surgery. A few weeks later, the patient underwent successful surgical resection, after which symptoms promptly resolved. Pathology report later confirmed an atypical lung carcinoid tumor. The patient remained in remission at 1-year follow-up.</div></div><div><h3>Discussion</h3><div>Medical therapy aids in managing severe hypercortisolism in ACTH-secreting tumors until definitive surgical treatment can be undertaken.</div></div><div><h3>Conclusion</h3><div>This case underscores the critical importance of promptly recognizing EAS and the resulting severe hypercortisolism symptoms because early surgical intervention can lead to a cure.</div></div>","PeriodicalId":7051,"journal":{"name":"AACE Clinical Case Reports","volume":"11 1","pages":"Pages 10-13"},"PeriodicalIF":1.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784622/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AACE Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2376060524001007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background/Objective
Cushing syndrome resulting from ectopic adrenocorticotropic hormone (ACTH) secretion (EAS) is a rare condition, and its occurrence in adolescents is even more uncommon, representing <1% of cases. We describe a case of EAS from a lung carcinoid tumor leading to Cushing syndrome in a young woman, which was successfully treated with excision of the tumor.
Case Report
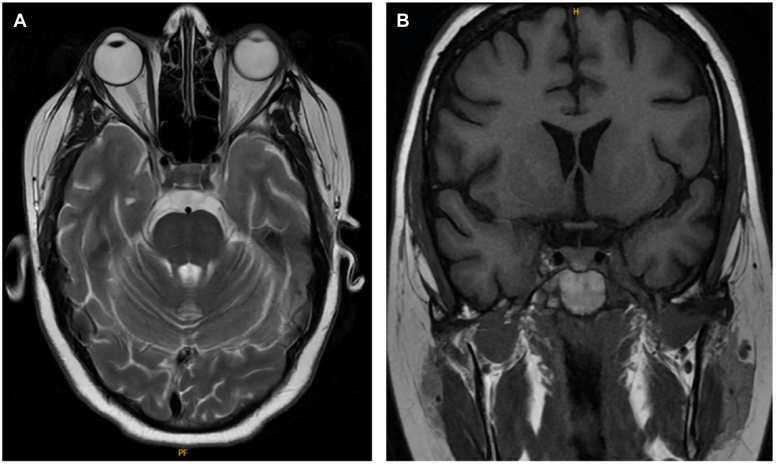
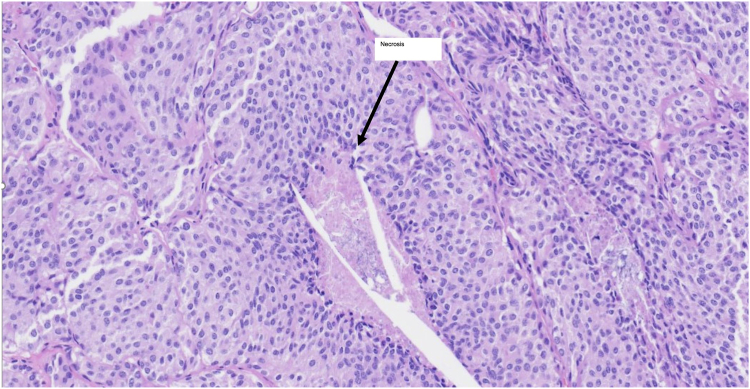
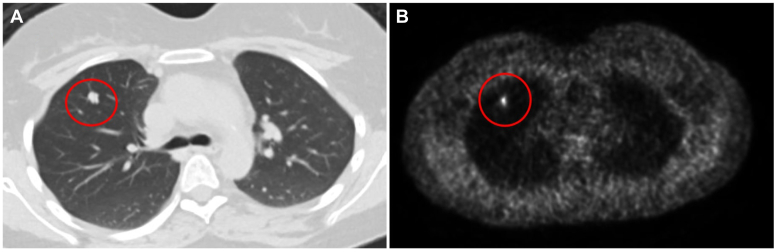
An 18-year-old woman presented with mood disturbances, weight gain, and fatigue for 6 months. Workup revealed high levels of urinary free cortisol (>900 μg/dL; normal range, <45 μg/dL) and midnight salivary cortisol (0.755 μg/dL; normal range, <0.09 μg/dL). The ACTH and cortisol levels remained elevated after a low-dose dexamethasone suppression test. Magnetic resonance imaging of the pituitary gland did not reveal any adenoma and inferior petrosal sinus sampling showed no central-to-peripheral gradient. A diagnosis of EAS was made. Subsequent body imaging noted a 1-cm lung nodule. Due to symptoms of severe hypercortisolism including hypokalemia and worsening mood changes, the patient was started on metyrapone as a bridge to surgery. A few weeks later, the patient underwent successful surgical resection, after which symptoms promptly resolved. Pathology report later confirmed an atypical lung carcinoid tumor. The patient remained in remission at 1-year follow-up.
Discussion
Medical therapy aids in managing severe hypercortisolism in ACTH-secreting tumors until definitive surgical treatment can be undertaken.
Conclusion
This case underscores the critical importance of promptly recognizing EAS and the resulting severe hypercortisolism symptoms because early surgical intervention can lead to a cure.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
