{"title":"Effect of Hematopoietic Stem Cell Transplantation Regimen on Tacrolimus Pharmacokinetics","authors":"Haruno Oku BS , Saki Yoshida BS , Takumi Hotta BS , Hirohito Muroi BS , Keizo Fukushima PhD , Kei Irie PhD , Tatsuya Hirano BS , Yoshimitsu Shimomura MD , Takayuki Ishikawa MD, PhD , Hiroaki Ikesue PhD , Nobuyuki Muroi PhD , Tohru Hashida PhD , Nobuyuki Sugioka PhD","doi":"10.1016/j.curtheres.2024.100775","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><div>Treatment with tacrolimus requires strict control of the whole-blood concentration in patients undergoing allogeneic hematopoietic stem cell transplantation (HSCT). In patients undergoing cord blood transplantation (CBT), there is a negative correlation between volume of distribution of tacrolimus and hemoglobin levels, which reflect the red blood cell (RBC) count. In this study, we evaluated the influence of the conditioning regimen (myeloablative and reduced-intensity conditioning) or donor source (cord blood, bone marrow, and peripheral blood stem cells) on the pharmacokinetics of tacrolimus in patients undergoing HSCT, including those undergoing CBT. We also examined applicability of dosing strategy of tacrolimus considering the RBC count.</div></div><div><h3>Methods</h3><div>We retrospectively analyzed clinical data—including whole-blood tacrolimus concentrations—from patients with HSCT. The observation period spanned from first continuous intravenous infusions until switch to oral medication, transfer to another hospital, relapse, or death. Population pharmacokinetic analysis was performed on whole-blood tacrolimus concentrations obtained from therapeutic drug monitoring during the observation period. Patient characteristics and laboratory data were evaluated as covariates.</div></div><div><h3>Results</h3><div>We enrolled 91 patients undergoing HSCT (CBT: <em>n</em> = 56; bone marrow transplantation: <em>n</em> = 22; and peripheral blood stem cell transplantation: <em>n</em> = 13); 58 and 33 patients received myeloablative conditioning and reduced-intensity conditioning, respectively. Whole-blood tacrolimus concentrations were accurately captured (<em>n</em> = 1,658 measurements) using a one-compartment and additive error model. The conditioning regimen and donor source did not have an impact on the pharmacokinetics of tacrolimus. Therefore, these factors were not considered when forming the dosing strategy. Nevertheless, a negative correlation between volume of distribution and hemoglobin level was confirmed, indicating that monitoring the RBC count is useful in assessing the dosing strategy.</div></div><div><h3>Conclusions</h3><div>A tacrolimus dosing strategy that considers the variability in hemoglobin levels applies to all patients undergoing HSCT.</div></div>","PeriodicalId":10920,"journal":{"name":"Current Therapeutic Research-clinical and Experimental","volume":"102 ","pages":"Article 100775"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11788801/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Therapeutic Research-clinical and Experimental","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0011393X24000456","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/27 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives
Treatment with tacrolimus requires strict control of the whole-blood concentration in patients undergoing allogeneic hematopoietic stem cell transplantation (HSCT). In patients undergoing cord blood transplantation (CBT), there is a negative correlation between volume of distribution of tacrolimus and hemoglobin levels, which reflect the red blood cell (RBC) count. In this study, we evaluated the influence of the conditioning regimen (myeloablative and reduced-intensity conditioning) or donor source (cord blood, bone marrow, and peripheral blood stem cells) on the pharmacokinetics of tacrolimus in patients undergoing HSCT, including those undergoing CBT. We also examined applicability of dosing strategy of tacrolimus considering the RBC count.
Methods
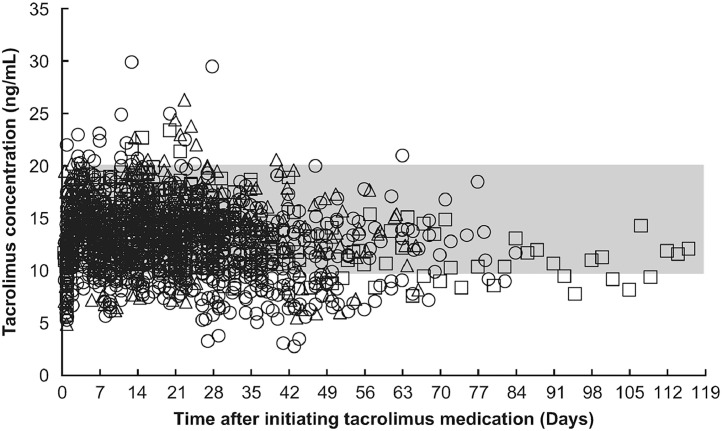
We retrospectively analyzed clinical data—including whole-blood tacrolimus concentrations—from patients with HSCT. The observation period spanned from first continuous intravenous infusions until switch to oral medication, transfer to another hospital, relapse, or death. Population pharmacokinetic analysis was performed on whole-blood tacrolimus concentrations obtained from therapeutic drug monitoring during the observation period. Patient characteristics and laboratory data were evaluated as covariates.
Results
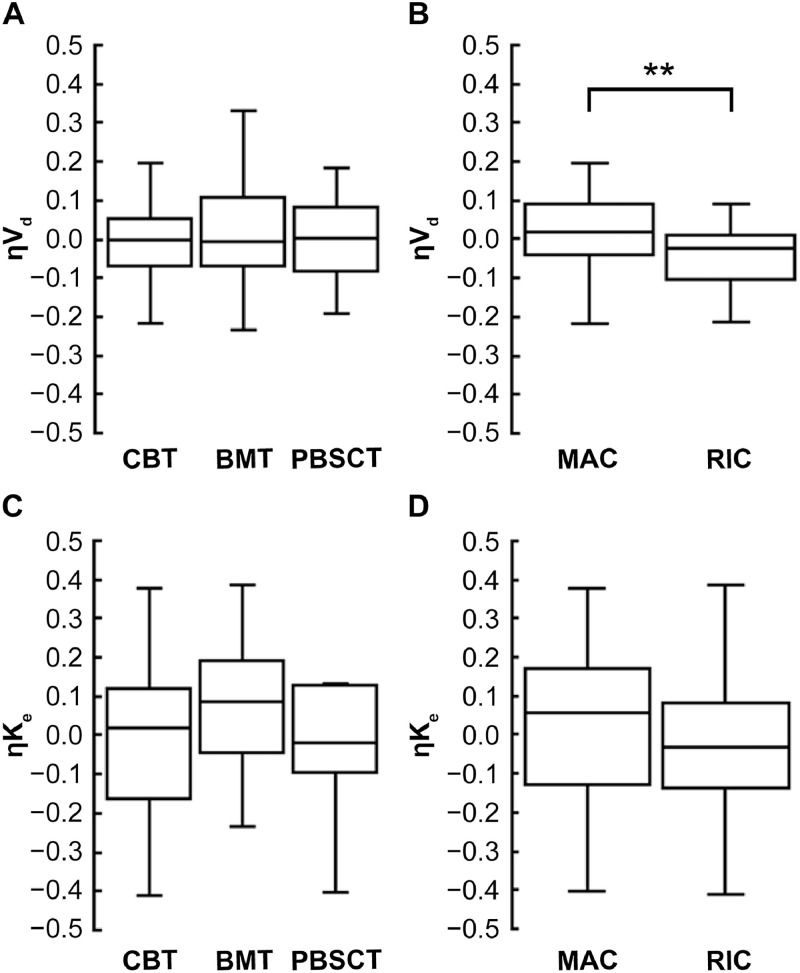
We enrolled 91 patients undergoing HSCT (CBT: n = 56; bone marrow transplantation: n = 22; and peripheral blood stem cell transplantation: n = 13); 58 and 33 patients received myeloablative conditioning and reduced-intensity conditioning, respectively. Whole-blood tacrolimus concentrations were accurately captured (n = 1,658 measurements) using a one-compartment and additive error model. The conditioning regimen and donor source did not have an impact on the pharmacokinetics of tacrolimus. Therefore, these factors were not considered when forming the dosing strategy. Nevertheless, a negative correlation between volume of distribution and hemoglobin level was confirmed, indicating that monitoring the RBC count is useful in assessing the dosing strategy.
Conclusions
A tacrolimus dosing strategy that considers the variability in hemoglobin levels applies to all patients undergoing HSCT.
期刊介绍:
We also encourage the submission of manuscripts presenting preclinical and very preliminary research that may stimulate further investigation of potentially relevant findings, as well as in-depth review articles on specific therapies or disease states, and applied health delivery or pharmacoeconomics.
CTR encourages and supports the submission of manuscripts describing:
• Interventions designed to understand or improve human health, disease treatment or disease prevention;
• Studies that focus on problems that are uncommon in resource-rich countries;
• Research that is "under-published" because of limited access to monetary resources such as English language support and Open Access fees (CTR offers deeply discounted English language editing);
• Republication of articles previously published in non-English journals (eg, evidence-based guidelines) which could be useful if translated into English;
• Preclinical and clinical product development studies that are not pursued for further investigation based upon early phase results.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
