Aleksander Osiowski, Kacper Stolarz, Dominik Taterra
{"title":"How can you manage an indomethacin-responsive headache in someone who cannot take indomethacin?","authors":"Aleksander Osiowski, Kacper Stolarz, Dominik Taterra","doi":"10.1097/WCO.0000000000001347","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>Paroxysmal hemicrania and hemicrania continua are rare primary headache disorders which are distinguished by an absolute response to indomethacin. As a matter of importance, no guidelines have been proposed for alternative therapeutic options in case of indomethacin intolerance. The purpose of this review is to provide an update on the current findings, especially focusing on the past 18 months, in the treatment of both paroxysmal hemicrania and hemicrania continua and to provide proposed management recommendations based on summarized evidence.</p><p><strong>Recent findings: </strong>Apart from well recognized gastrolesive effects of indomethacin, a substantial number of patients may suffer from neuropsychiatric adverse reactions. Recent studies demonstrated that melatonin, which has been known for its effectiveness for hemicrania continua, is also useful for paroxysmal hemicrania. Promising nonpharmacological treatment option, which is noninvasive vagus nerve stimulation, has been shown to be beneficial for both indomethacin-responsive headache disorders allowing the reduction of indomethacin dosage. Although the data on substitutive medication choice for indomethacin are currently scarce, the most consistent results have been repeatedly achieved with acemethacin, selective COX-2 inhibitors, and anticonvulsants. However, considering the crucial role of pathophysiology, research investigating the efficacy of drugs targeting the trigemino-vascular system activation, as well as controlled trials assessing the efficacy involving the aforementioned therapeutic options are still vague.</p><p><strong>Summary: </strong>In spite of numerous reports suggesting reliable alternatives to indomethacin, the consensus on pharmacological therapy guidelines for indomethacin-responsive headache disorders has not yet been reached. Further research and agreement from the experts' standpoint are needed for an establishment of reliable treatment recommendations.</p>","PeriodicalId":11059,"journal":{"name":"Current Opinion in Neurology","volume":" ","pages":"254-261"},"PeriodicalIF":4.4000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12052051/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Opinion in Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/WCO.0000000000001347","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/5 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
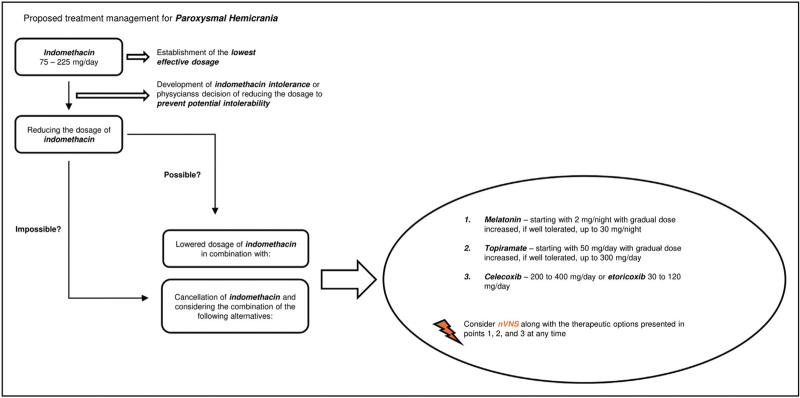
Purpose of review: Paroxysmal hemicrania and hemicrania continua are rare primary headache disorders which are distinguished by an absolute response to indomethacin. As a matter of importance, no guidelines have been proposed for alternative therapeutic options in case of indomethacin intolerance. The purpose of this review is to provide an update on the current findings, especially focusing on the past 18 months, in the treatment of both paroxysmal hemicrania and hemicrania continua and to provide proposed management recommendations based on summarized evidence.
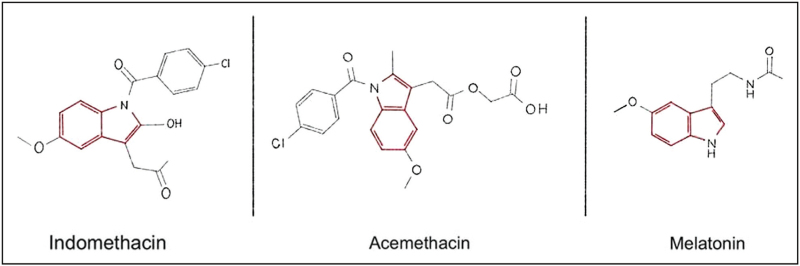
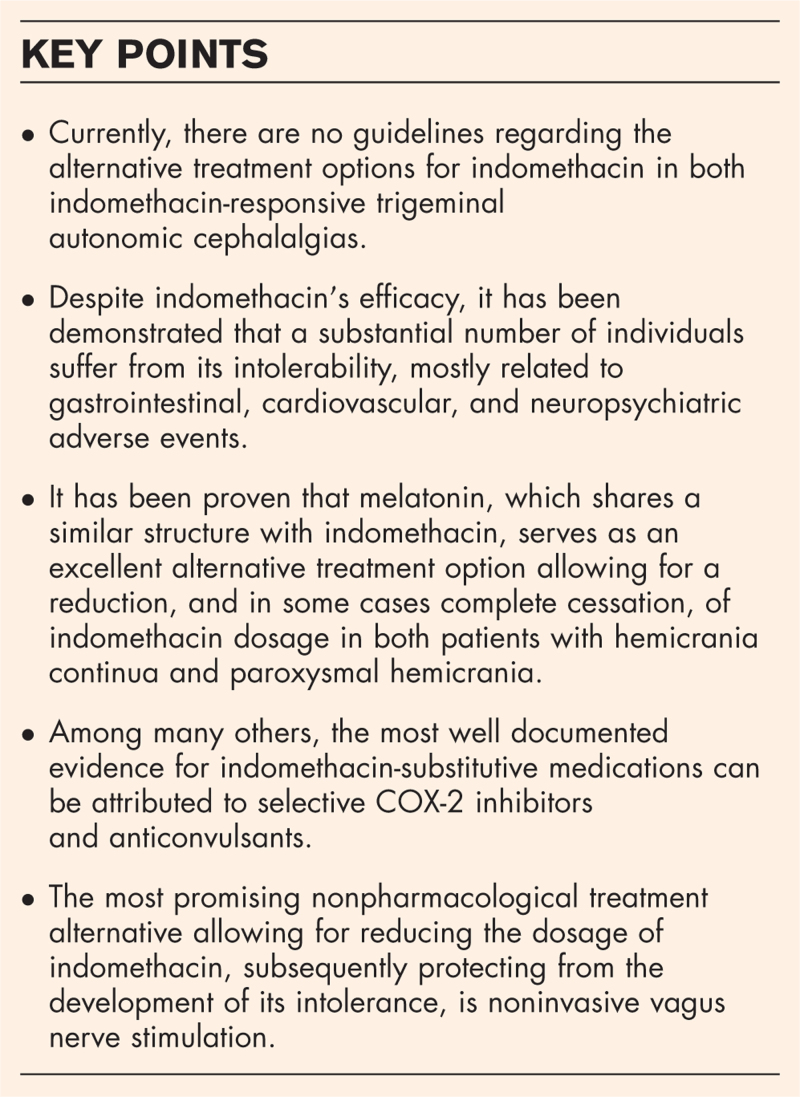
Recent findings: Apart from well recognized gastrolesive effects of indomethacin, a substantial number of patients may suffer from neuropsychiatric adverse reactions. Recent studies demonstrated that melatonin, which has been known for its effectiveness for hemicrania continua, is also useful for paroxysmal hemicrania. Promising nonpharmacological treatment option, which is noninvasive vagus nerve stimulation, has been shown to be beneficial for both indomethacin-responsive headache disorders allowing the reduction of indomethacin dosage. Although the data on substitutive medication choice for indomethacin are currently scarce, the most consistent results have been repeatedly achieved with acemethacin, selective COX-2 inhibitors, and anticonvulsants. However, considering the crucial role of pathophysiology, research investigating the efficacy of drugs targeting the trigemino-vascular system activation, as well as controlled trials assessing the efficacy involving the aforementioned therapeutic options are still vague.
Summary: In spite of numerous reports suggesting reliable alternatives to indomethacin, the consensus on pharmacological therapy guidelines for indomethacin-responsive headache disorders has not yet been reached. Further research and agreement from the experts' standpoint are needed for an establishment of reliable treatment recommendations.
期刊介绍:
Current Opinion in Neurology is a highly regarded journal offering insightful editorials and on-the-mark invited reviews; covering key subjects such as cerebrovascular disease, developmental disorders, neuroimaging and demyelinating diseases. Published bimonthly, each issue of Current Opinion in Neurology introduces world renowned guest editors and internationally recognized academics within the neurology field, delivering a widespread selection of expert assessments on the latest developments from the most recent literature.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
