In-Hospital Pulmonary Thromboembolism Development by Disease at Admission - A Nationwide, Retrospective, Observational Study Using Japanese Claims Data.
{"title":"In-Hospital Pulmonary Thromboembolism Development by Disease at Admission - A Nationwide, Retrospective, Observational Study Using Japanese Claims Data.","authors":"Ken-Ichi Hiasa, Miki Imura, Susumu Hirose","doi":"10.1253/circrep.CR-24-0140","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prevention of death from in-hospital pulmonary thromboembolism (PE) is crucial, but research exploring the risk factors for this event remains limited.</p><p><strong>Methods and results: </strong>This retrospective analysis evaluated PE data among hospitalized patients, focusing on the diseases present on admission to hospital with the highest number of patients with in-hospital PE events, using the Medical Data Vision database (January 2017-December 2021). Endpoints included the incidence rate of in-hospital PE, patient characteristics, and PE prophylactic procedures. Overall, 4,684,659 patients (in-hospital PE cohort, n=5,007; non-PE cohort, n=4,679,952) were eligible: heart failure (n=208; n=87,160), femoral fracture (n=478; n=139,049), pneumonia (n=309; n=222,257), stroke (n=351; n=248,805), and cancer (n=934; n=764,413). The incidence rate of in-hospital PE in the overall population was 20.6/1,000 person-years: heart failure (34.6), femoral fracture (35.3), pneumonia (21.4), stroke (15.9), and cancer (25.6). History of venous thromboembolism (VTE) was a risk factor for in-hospital PE in >50% of patients in all subgroups. Prophylactic PE procedures were implemented in 33.8% of the overall population: femoral fracture (79.5%), cancer (49.7%), stroke (24.2%), heart failure (12.7%), and pneumonia (6.2%).</p><p><strong>Conclusions: </strong>The incidence of in-hospital PE was not high overall but was higher in patients with a history of VTE and those with hospitalization due to heart failure or femoral fracture. Risk assessment for in-hospital PE, including medical history and diagnosis at admission, is preferred in hospitalized patients.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 2","pages":"66-75"},"PeriodicalIF":1.1000,"publicationDate":"2025-01-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11807694/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-24-0140","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prevention of death from in-hospital pulmonary thromboembolism (PE) is crucial, but research exploring the risk factors for this event remains limited.
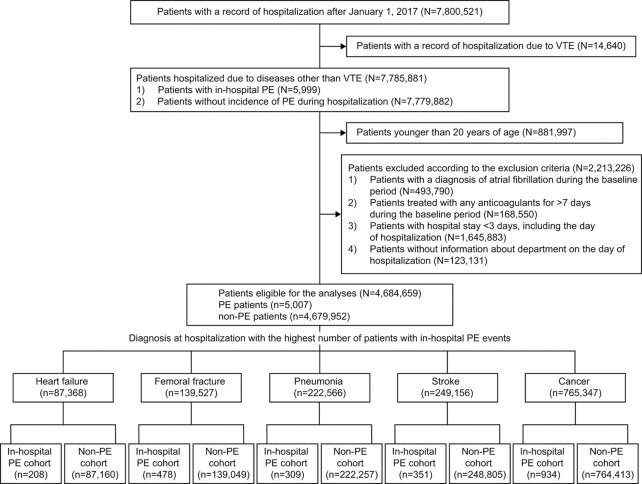
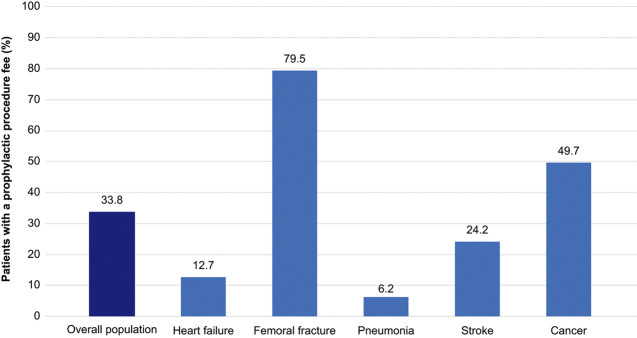
Methods and results: This retrospective analysis evaluated PE data among hospitalized patients, focusing on the diseases present on admission to hospital with the highest number of patients with in-hospital PE events, using the Medical Data Vision database (January 2017-December 2021). Endpoints included the incidence rate of in-hospital PE, patient characteristics, and PE prophylactic procedures. Overall, 4,684,659 patients (in-hospital PE cohort, n=5,007; non-PE cohort, n=4,679,952) were eligible: heart failure (n=208; n=87,160), femoral fracture (n=478; n=139,049), pneumonia (n=309; n=222,257), stroke (n=351; n=248,805), and cancer (n=934; n=764,413). The incidence rate of in-hospital PE in the overall population was 20.6/1,000 person-years: heart failure (34.6), femoral fracture (35.3), pneumonia (21.4), stroke (15.9), and cancer (25.6). History of venous thromboembolism (VTE) was a risk factor for in-hospital PE in >50% of patients in all subgroups. Prophylactic PE procedures were implemented in 33.8% of the overall population: femoral fracture (79.5%), cancer (49.7%), stroke (24.2%), heart failure (12.7%), and pneumonia (6.2%).
Conclusions: The incidence of in-hospital PE was not high overall but was higher in patients with a history of VTE and those with hospitalization due to heart failure or femoral fracture. Risk assessment for in-hospital PE, including medical history and diagnosis at admission, is preferred in hospitalized patients.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
