{"title":"An Adverse Double-Hit by Pembrolizumab: A Case Report of Bullous Pemphigoid and Pneumonitis.","authors":"Christodoulos Chatzigrigoriadis, Prodromos Avramidis, Christos Davoulos, Foteinos-Ioannis Dimitrakopoulos, George Eleftherakis, Christina Petropoulou, Despoina Sperdouli, Georgios Marios Stergiopoulos, Panagis Galiatsatos, Stelios Assimakopoulos","doi":"10.14740/jmc5089","DOIUrl":null,"url":null,"abstract":"<p><p>Immune checkpoint inhibitors like pembrolizumab represent a modern approach to the management of various malignancies, including non-small cell lung cancer. The therapeutic activity of immunotherapy is exerted by the activation of immune cells against the tumor cells. However, systemic activation of the immune system can lead to the development of autoimmune complications known as immune-related adverse events. A combination of rare immune-related adverse events is occasionally observed simultaneously in the same patient. We present the case of a 66-year-old male with squamous non-small cell lung carcinoma who presented to the emergency department with dyspnea and respiratory failure. Imaging findings were consistent with pulmonary embolism and nonspecific interstitial pneumonitis. One month before this event, he was diagnosed with bullous pemphigoid following 21 cycles of treatment with pembrolizumab. The radiological findings, the lack of response to antibiotics, the negative microbiological workup, and the excellent response to corticosteroids established the diagnosis of pembrolizumab-induced pneumonitis. The combination of bullous pemphigoid and pneumonitis secondary to pembrolizumab is rare; only a few case reports exist in the literature. Hence, this case highlights the possibility of multiple immune-related adverse events in the same patient. The exclusion of infectious diseases and other immunologic disorders with a similar clinical presentation is necessary to make the final diagnosis of immune-related adverse events and start the appropriate treatment. Serology, histopathology, and direct immunofluorescence aid to the diagnosis of immune-related bullous pemphigoid; the differential diagnosis includes other pemphigoid or lichenoid diseases, Stevens-Johnson syndrome/toxic epidermal necrolysis, and drug reaction with eosinophilia and systemic symptoms. Imaging, microbiological testing, and bronchoscopy (if possible) confirm the diagnosis of immune-related pneumonitis, which should be differentiated from acute coronary syndrome, cardiogenic pulmonary edema, pulmonary embolism, tumor progression, and lower respiratory tract infections (especially <i>Pneumocystis jirovecii</i> pneumonia in immunocompromised patients). An interdisciplinary approach is necessary for the management of these cases.</p>","PeriodicalId":101328,"journal":{"name":"Journal of medical cases","volume":"16 2","pages":"69-76"},"PeriodicalIF":0.9000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809608/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of medical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc5089","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/2 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
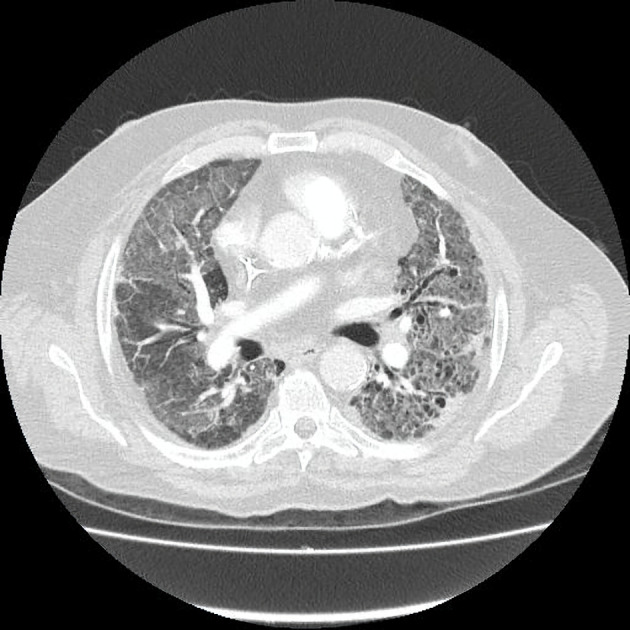
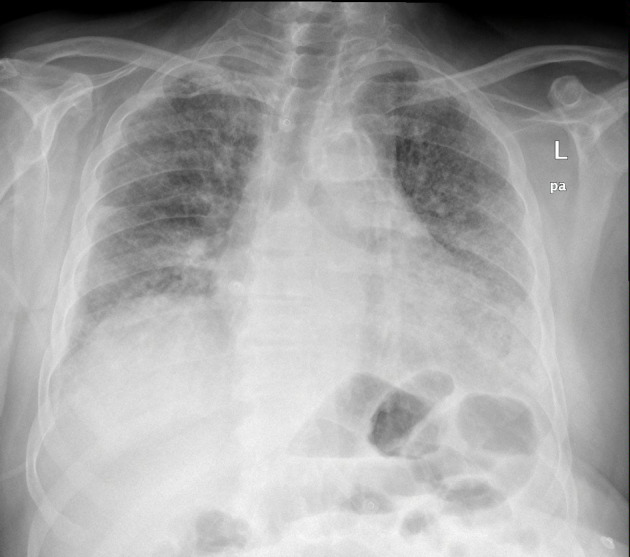
Immune checkpoint inhibitors like pembrolizumab represent a modern approach to the management of various malignancies, including non-small cell lung cancer. The therapeutic activity of immunotherapy is exerted by the activation of immune cells against the tumor cells. However, systemic activation of the immune system can lead to the development of autoimmune complications known as immune-related adverse events. A combination of rare immune-related adverse events is occasionally observed simultaneously in the same patient. We present the case of a 66-year-old male with squamous non-small cell lung carcinoma who presented to the emergency department with dyspnea and respiratory failure. Imaging findings were consistent with pulmonary embolism and nonspecific interstitial pneumonitis. One month before this event, he was diagnosed with bullous pemphigoid following 21 cycles of treatment with pembrolizumab. The radiological findings, the lack of response to antibiotics, the negative microbiological workup, and the excellent response to corticosteroids established the diagnosis of pembrolizumab-induced pneumonitis. The combination of bullous pemphigoid and pneumonitis secondary to pembrolizumab is rare; only a few case reports exist in the literature. Hence, this case highlights the possibility of multiple immune-related adverse events in the same patient. The exclusion of infectious diseases and other immunologic disorders with a similar clinical presentation is necessary to make the final diagnosis of immune-related adverse events and start the appropriate treatment. Serology, histopathology, and direct immunofluorescence aid to the diagnosis of immune-related bullous pemphigoid; the differential diagnosis includes other pemphigoid or lichenoid diseases, Stevens-Johnson syndrome/toxic epidermal necrolysis, and drug reaction with eosinophilia and systemic symptoms. Imaging, microbiological testing, and bronchoscopy (if possible) confirm the diagnosis of immune-related pneumonitis, which should be differentiated from acute coronary syndrome, cardiogenic pulmonary edema, pulmonary embolism, tumor progression, and lower respiratory tract infections (especially Pneumocystis jirovecii pneumonia in immunocompromised patients). An interdisciplinary approach is necessary for the management of these cases.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
