Juan David Niño-Calvera, Julian Senosiain, Nicolas Nuñez-Ordonez, Ivonne Pineda, Lina Ramírez, Carlos Villa, Carlos Obando, Tomas Chalela, Nestor Sandoval, Juan P Umaña, Jaime Camacho
{"title":"Total Arch Replacement is Safe as Hemiarch Repair in Acute Type A Aortic Dissection in a Middle-Income Country Setting.","authors":"Juan David Niño-Calvera, Julian Senosiain, Nicolas Nuñez-Ordonez, Ivonne Pineda, Lina Ramírez, Carlos Villa, Carlos Obando, Tomas Chalela, Nestor Sandoval, Juan P Umaña, Jaime Camacho","doi":"10.21470/1678-9741-2024-0088","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectiver: </strong>The aim of this study was to determine the clinical outcomes of patients with acute type A aortic dissection comparing proximal aortic repair vs. total arch replacement.</p><p><strong>Methods: </strong>This was a retrospective cohort study. We included all acute type A aortic dissection procedures from January 2002 to November 2022. Groups were defined according to the extent of aortic replacement (hemiarch repair vs. total arch replacement). We collected data from pre, intra, and postoperative variables. Our main endpoints were stroke rate, spinal cord injury, and in-hospital mortality. We performed a statistical analysis for between-group comparisons according to the nature and distribution of variables. Bivariate analyses were done using the Mann-Whitney U test and for categorical variables, the Chi-square test or Fisher's exact test. Significance was established at alpha level of 0.05.</p><p><strong>Results: </strong>We identified 107 acute type A aortic dissection procedures (69 hemiarch repairs vs. 38 total arch replacements). There were no differences in postoperative outcomes such as surgical site infection or acute kidney injury. Bleeding reoperation was more frequent in the hemiarch group (30% vs. 11 %). We did not find statistically significant differences in stroke rate, spinal cord injury, or in-hospital mortality.</p><p><strong>Conclusion: </strong>Acute type A aortic dissection treatment is still a challenge. Total arch replacement does not increase the risk of major early postoperative complications in comparison to hemiarch repair. The extended repair seems to provide benefits such as a lower risk of reoperation. Total arch replacement should be performed in selected patients, as it may improve long-term outcomes.</p>","PeriodicalId":72457,"journal":{"name":"Brazilian journal of cardiovascular surgery","volume":"40 1","pages":"e20240088"},"PeriodicalIF":1.2000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11817151/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brazilian journal of cardiovascular surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21470/1678-9741-2024-0088","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectiver: The aim of this study was to determine the clinical outcomes of patients with acute type A aortic dissection comparing proximal aortic repair vs. total arch replacement.
Methods: This was a retrospective cohort study. We included all acute type A aortic dissection procedures from January 2002 to November 2022. Groups were defined according to the extent of aortic replacement (hemiarch repair vs. total arch replacement). We collected data from pre, intra, and postoperative variables. Our main endpoints were stroke rate, spinal cord injury, and in-hospital mortality. We performed a statistical analysis for between-group comparisons according to the nature and distribution of variables. Bivariate analyses were done using the Mann-Whitney U test and for categorical variables, the Chi-square test or Fisher's exact test. Significance was established at alpha level of 0.05.
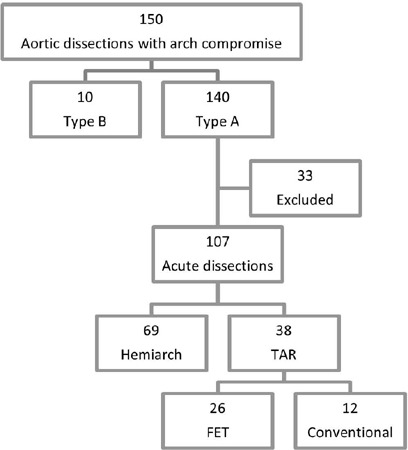
Results: We identified 107 acute type A aortic dissection procedures (69 hemiarch repairs vs. 38 total arch replacements). There were no differences in postoperative outcomes such as surgical site infection or acute kidney injury. Bleeding reoperation was more frequent in the hemiarch group (30% vs. 11 %). We did not find statistically significant differences in stroke rate, spinal cord injury, or in-hospital mortality.
Conclusion: Acute type A aortic dissection treatment is still a challenge. Total arch replacement does not increase the risk of major early postoperative complications in comparison to hemiarch repair. The extended repair seems to provide benefits such as a lower risk of reoperation. Total arch replacement should be performed in selected patients, as it may improve long-term outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
