Kyotaro Koshika, Wataru Hashimoto, Ai Nakakuki, Kanako Yajima, Tatsuya Ichinohe
{"title":"Comparative efficacy of different video laryngoscopy types in difficult tracheal intubation cases: a randomized crossover manikin study.","authors":"Kyotaro Koshika, Wataru Hashimoto, Ai Nakakuki, Kanako Yajima, Tatsuya Ichinohe","doi":"10.17245/jdapm.2025.25.1.33","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Video laryngoscopy is beneficial in difficult airway intubation; however, various factors complicate the process. These devices come in different designs, and their usefulness may vary by type. In this study, we compared the effectiveness of several video laryngoscopic. instruments across three simulated difficult intubation scenarios using manikin models.</p><p><strong>Methods: </strong>Training simulators for tracheal intubation were set to four conditions: (i) Normal (mouth opening: 50 mm, normal neck); (ii) Head tilt disorder (mouth opening: 50 mm, rigid neck); (iii) Trismus (mouth opening: 20 mm, normal neck); and (iv) Head tilt disorder + trismus (mouth opening: 20 mm, rigid neck). Seventeen dental anesthesiologists attempted oral tracheal intubation using the following video laryngoscopes: Airway Scope; McGRATH (Normal blade [size 3]); McGRATH (X-blade); and i-view. Evaluated parameters included total intubation time, glottic visualization time, tube induction time, success rate, and difficulty grading of tracheal intubation (Cormack-Lehane classification and the Numerical Rating Scale [NRS]). Statistical analysis was conducted using mixed models, incorporating two-way ANOVA, Tukey's test, two-way ANOVA without repeated measures, and Kruskal-Wallis test, with P < 0.05 deemed statistically significant.</p><p><strong>Results: </strong>Intubation time using i-view was significantly longer for head tilt disorder and trismus compared to other video laryngoscopes (head tilt disorder: P < 0.001 for all, trismus: P = 0.021 vs. Airway Scope, P = 0.028 vs. X-blade). The Cormack-Lehane grade was notably high (P = 0.001) for tracheal intubation with i-view in the head tilt disorder scenario, with intubation failing in three cases. In the combined situation of head tilt disorder and trismus, intubation time with Airway Scope was shorter (P < 0.001 vs. X-blade), achieving a success rate of 100%. However, all attempts with i-view were unsuccessful. The NRS score was significantly higher for i-view compared to the other video laryngoscopes (P < 0.001).</p><p><strong>Conclusion: </strong>Video laryngoscopy effectiveness varies by type in difficult tracheal intubation cases. The Airway Scope or McGRATH instrument appears more suitable for such cases, as indicated by the metrics of intubation time, success rate, and difficulty level.</p>","PeriodicalId":94330,"journal":{"name":"Journal of dental anesthesia and pain medicine","volume":"25 1","pages":"33-42"},"PeriodicalIF":1.2000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11811514/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of dental anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17245/jdapm.2025.25.1.33","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Video laryngoscopy is beneficial in difficult airway intubation; however, various factors complicate the process. These devices come in different designs, and their usefulness may vary by type. In this study, we compared the effectiveness of several video laryngoscopic. instruments across three simulated difficult intubation scenarios using manikin models.
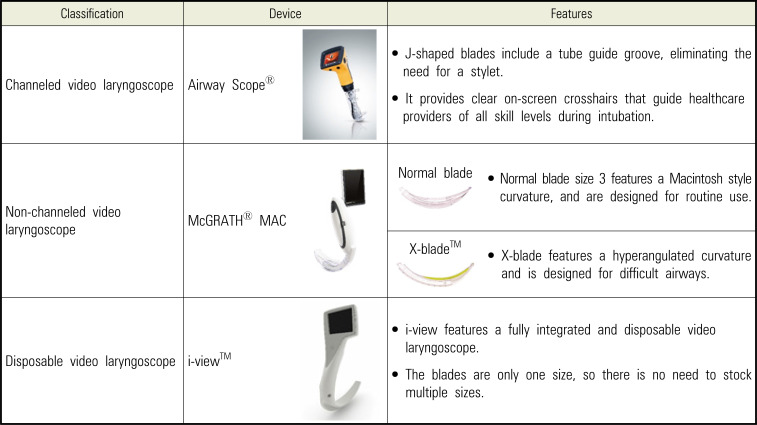
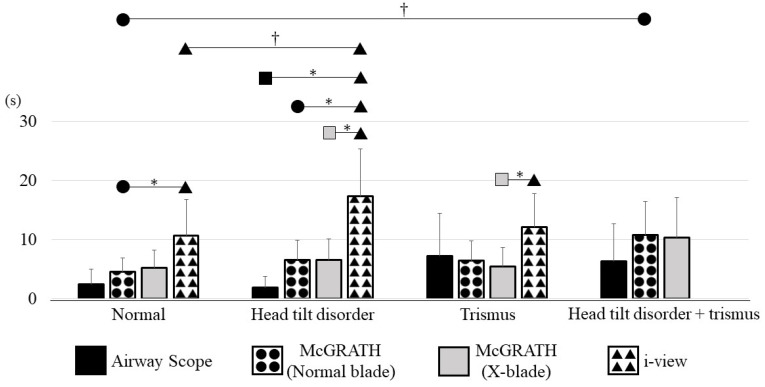
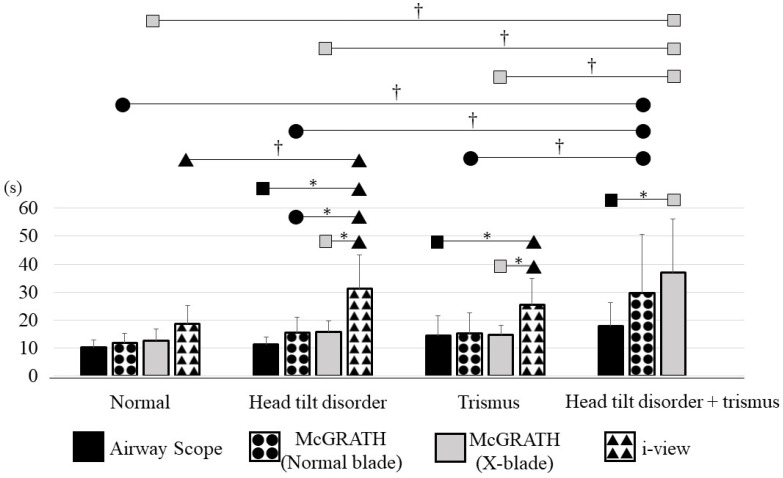
Methods: Training simulators for tracheal intubation were set to four conditions: (i) Normal (mouth opening: 50 mm, normal neck); (ii) Head tilt disorder (mouth opening: 50 mm, rigid neck); (iii) Trismus (mouth opening: 20 mm, normal neck); and (iv) Head tilt disorder + trismus (mouth opening: 20 mm, rigid neck). Seventeen dental anesthesiologists attempted oral tracheal intubation using the following video laryngoscopes: Airway Scope; McGRATH (Normal blade [size 3]); McGRATH (X-blade); and i-view. Evaluated parameters included total intubation time, glottic visualization time, tube induction time, success rate, and difficulty grading of tracheal intubation (Cormack-Lehane classification and the Numerical Rating Scale [NRS]). Statistical analysis was conducted using mixed models, incorporating two-way ANOVA, Tukey's test, two-way ANOVA without repeated measures, and Kruskal-Wallis test, with P < 0.05 deemed statistically significant.
Results: Intubation time using i-view was significantly longer for head tilt disorder and trismus compared to other video laryngoscopes (head tilt disorder: P < 0.001 for all, trismus: P = 0.021 vs. Airway Scope, P = 0.028 vs. X-blade). The Cormack-Lehane grade was notably high (P = 0.001) for tracheal intubation with i-view in the head tilt disorder scenario, with intubation failing in three cases. In the combined situation of head tilt disorder and trismus, intubation time with Airway Scope was shorter (P < 0.001 vs. X-blade), achieving a success rate of 100%. However, all attempts with i-view were unsuccessful. The NRS score was significantly higher for i-view compared to the other video laryngoscopes (P < 0.001).
Conclusion: Video laryngoscopy effectiveness varies by type in difficult tracheal intubation cases. The Airway Scope or McGRATH instrument appears more suitable for such cases, as indicated by the metrics of intubation time, success rate, and difficulty level.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
