Capacity assessment for EHR-based medical device post-market surveillance for synthetic mid-urethral slings among women with stress urinary incontinence: a NEST consortium study.
Michael E Matheny, Amy M Perkins, Kimberly Rieger-Christ, Joseph S Ross, Jialin Mao, Art Sedrakyan, Nilay D Shah, Robert Winter, W Stuart Reynolds, Arthur Mourtzinos, Wade L Schulz, Victoria Bartlett, Michael Solotke, Sameer Pandya, Suvekshya Aryal, Ahra Cho, Edward A Frankenberger, Daniel Park, Danielle Bostrom, Susan Robbins, Aron Yustein, Bilal Chughtai, Emanuel C Trabuco
{"title":"Capacity assessment for EHR-based medical device post-market surveillance for synthetic mid-urethral slings among women with stress urinary incontinence: a NEST consortium study.","authors":"Michael E Matheny, Amy M Perkins, Kimberly Rieger-Christ, Joseph S Ross, Jialin Mao, Art Sedrakyan, Nilay D Shah, Robert Winter, W Stuart Reynolds, Arthur Mourtzinos, Wade L Schulz, Victoria Bartlett, Michael Solotke, Sameer Pandya, Suvekshya Aryal, Ahra Cho, Edward A Frankenberger, Daniel Park, Danielle Bostrom, Susan Robbins, Aron Yustein, Bilal Chughtai, Emanuel C Trabuco","doi":"10.1136/bmjsit-2023-000193","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the feasibility for use of electronic health record (EHR) data in conducting adverse event surveillance among women who received mid-urethral slings (MUS) to treat stress urinary incontinence (SUI) in five health systems.</p><p><strong>Design: </strong>Retrospective observational study using EHR data from 2010 through 2021. Women with a history of MUS were identified using common data models; a common analytic code was executed at each site. A manual chart review was conducted in a per-site random patient subset to establish a reference standard. Automated text processing (Text Processed Integrated (TPI)) was developed and evaluated at each site to determine the surgical approach and synthetic mesh implantation. Patients were characterized and surgical outcomes were ascertained over 730 subsequent days.</p><p><strong>Setting: </strong>Five large tertiary care academic medical centers.</p><p><strong>Participants: </strong>Across five health systems, 9,906 eligible patients (mean age 57-60 per site) were identified.</p><p><strong>Main outcome measures: </strong>Determination of surgical approach, synthetic mesh implantation, and assessment of the duration of surveillance for mortality and reoperation rates following MUS implantation.</p><p><strong>Results: </strong>In the TPI cohort analysis, 3,331 patients were identified. Surgical approach per site was retropubic (42% to 77%), transobturator (6% to 44%), single incision (0% to 24%), and adjustable sling (0% to <4%). Concordance rates for TPI using chart review were 71%-90% at each site for the surgical approach and 28%-85% for synthetic mesh implantation. Patient follow-up observation rates for mortality and reoperation ranged from 22% to 36% at 90 days, 15% to 30% at 365 days, and 8% to 19% at 730 days.</p><p><strong>Conclusion: </strong>Using EHR data alone, identification of medical devices and surgical approaches was feasible among women with MUS surgery for SUI, but long-term follow-up ascertainment rates were low. Medical device surveillance using EHR data should be evaluated in the context of the clinical use case, as applicability may vary.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"7 1","pages":"e000193"},"PeriodicalIF":1.6000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11822424/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2023-000193","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To evaluate the feasibility for use of electronic health record (EHR) data in conducting adverse event surveillance among women who received mid-urethral slings (MUS) to treat stress urinary incontinence (SUI) in five health systems.
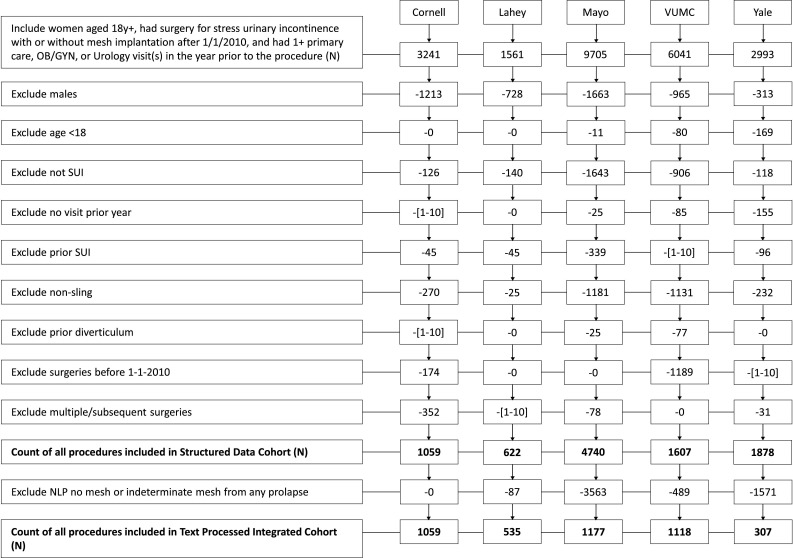
Design: Retrospective observational study using EHR data from 2010 through 2021. Women with a history of MUS were identified using common data models; a common analytic code was executed at each site. A manual chart review was conducted in a per-site random patient subset to establish a reference standard. Automated text processing (Text Processed Integrated (TPI)) was developed and evaluated at each site to determine the surgical approach and synthetic mesh implantation. Patients were characterized and surgical outcomes were ascertained over 730 subsequent days.
Setting: Five large tertiary care academic medical centers.
Participants: Across five health systems, 9,906 eligible patients (mean age 57-60 per site) were identified.
Main outcome measures: Determination of surgical approach, synthetic mesh implantation, and assessment of the duration of surveillance for mortality and reoperation rates following MUS implantation.
Results: In the TPI cohort analysis, 3,331 patients were identified. Surgical approach per site was retropubic (42% to 77%), transobturator (6% to 44%), single incision (0% to 24%), and adjustable sling (0% to <4%). Concordance rates for TPI using chart review were 71%-90% at each site for the surgical approach and 28%-85% for synthetic mesh implantation. Patient follow-up observation rates for mortality and reoperation ranged from 22% to 36% at 90 days, 15% to 30% at 365 days, and 8% to 19% at 730 days.
Conclusion: Using EHR data alone, identification of medical devices and surgical approaches was feasible among women with MUS surgery for SUI, but long-term follow-up ascertainment rates were low. Medical device surveillance using EHR data should be evaluated in the context of the clinical use case, as applicability may vary.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
