Distribution and failure patterns of primary central nervous system lymphoma related to the hippocampus: implications for hippocampal avoidance irradiation.
Hyejo Ryu, Xue Li, Tae Hoon Lee, Tae Min Kim, Seung Hong Choi, Chul-Kee Park, Soon Tae Lee, Sung-Hye Park, Jae-Kyung Won, Bum-Sup Jang, Il Han Kim, Joo Ho Lee
{"title":"Distribution and failure patterns of primary central nervous system lymphoma related to the hippocampus: implications for hippocampal avoidance irradiation.","authors":"Hyejo Ryu, Xue Li, Tae Hoon Lee, Tae Min Kim, Seung Hong Choi, Chul-Kee Park, Soon Tae Lee, Sung-Hye Park, Jae-Kyung Won, Bum-Sup Jang, Il Han Kim, Joo Ho Lee","doi":"10.1007/s11060-025-04965-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Hippocampal injury from WBRT contributes to neurocognitive decline in brain malignancy patients. HA-WBRT may mitigate this by reducing hippocampal radiation exposure, but its feasibility in PCNSL remains unassessed regarding hippocampal involvement and failure rates. This study evaluates hippocampal involvement at diagnosis and after treatment in PCNSL patients.</p><p><strong>Materials and methods: </strong>We conducted a retrospective analysis of 278 immunocompetent PCNSL patients diagnosed between 2000 and 2021. Following high-dose methotrexate-based induction chemotherapy, patients either received consolidation therapy, including RT, cytarabine alone, or autologous stem cell transplantation or underwent observation. Hippocampus was outlined on T1 MRI images and expanded by a 5 mm margin to create the hippocampal avoidance region (HAR). Hippocampal failure was defined as recurrence or progression at HAR. The median follow-up was 38.7 months (range 3.1-239.4 months).</p><p><strong>Results: </strong>Of the 278 patients diagnosed with PCNSL, 39.9% presented initial lesions at HAR. After induction therapy, 212 evaluable patients received consolidation treatments or observation. Intracranial failures occurred in 47.6% (n = 101), with 66.3% (n = 67) occurring outside the HAR and 33.7% (n = 34) inside the HAR. Unifocal disease (HR 0.61, 95% CI 0.39-0.96, p = 0.025) was associated with a lower risk of hippocampal failures, while initial HAR involvement significantly increased the risk (HR 2.26, 95% CI 1.18-4.47, p = 0.018). Patients with unifocal disease outside the HAR had the lowest 3-year hippocampal failure rate (6.2%). RT that included the hippocampus did not significantly affect hippocampal failure rates in patients without initial HAR lesions (p = 0.282), with three-year rates of 9.2 vs. 14.6% for other treatments. However, among patients with initial HAR involvement, RT including the hippocampus significantly reduced hippocampal failure rates compared to other approaches (p = 0.002). Hippocampal failure rates were comparable, with conventional WBRT at 14.6% and HA-WBRT at 19% in patients without initial HAR lesions (p = 0.734).</p><p><strong>Conclusion: </strong>The routine application of the HA-WBRT strategy is not supported due to the high risk of hippocampal failures in general and requires further investigation to establish its feasibility and safety in well-defined subgroups. Our results suggest that the HA-WBRT strategy could be evaluated for select PCNSL patients with unifocal lesions or those located outside the HAR.</p>","PeriodicalId":16425,"journal":{"name":"Journal of Neuro-Oncology","volume":" ","pages":"95-104"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12041158/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neuro-Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11060-025-04965-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Hippocampal injury from WBRT contributes to neurocognitive decline in brain malignancy patients. HA-WBRT may mitigate this by reducing hippocampal radiation exposure, but its feasibility in PCNSL remains unassessed regarding hippocampal involvement and failure rates. This study evaluates hippocampal involvement at diagnosis and after treatment in PCNSL patients.
Materials and methods: We conducted a retrospective analysis of 278 immunocompetent PCNSL patients diagnosed between 2000 and 2021. Following high-dose methotrexate-based induction chemotherapy, patients either received consolidation therapy, including RT, cytarabine alone, or autologous stem cell transplantation or underwent observation. Hippocampus was outlined on T1 MRI images and expanded by a 5 mm margin to create the hippocampal avoidance region (HAR). Hippocampal failure was defined as recurrence or progression at HAR. The median follow-up was 38.7 months (range 3.1-239.4 months).
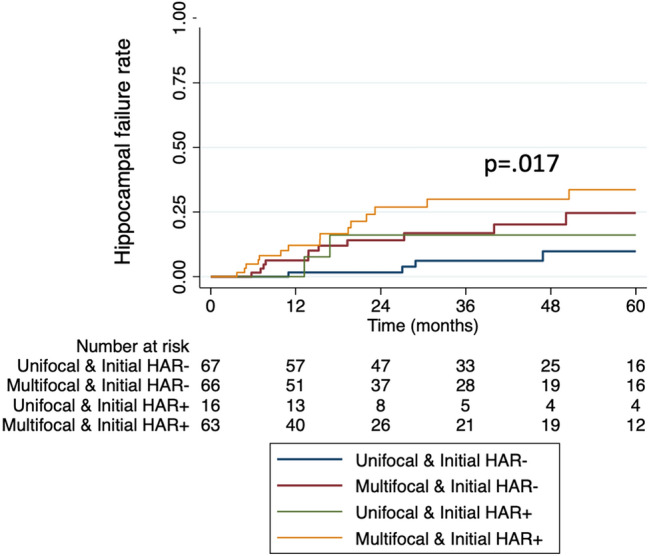
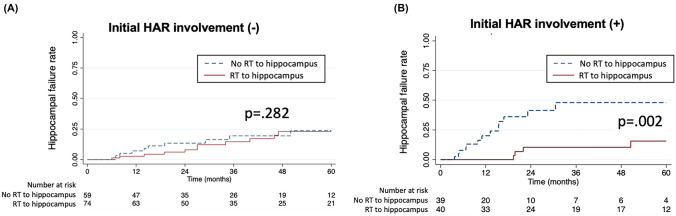
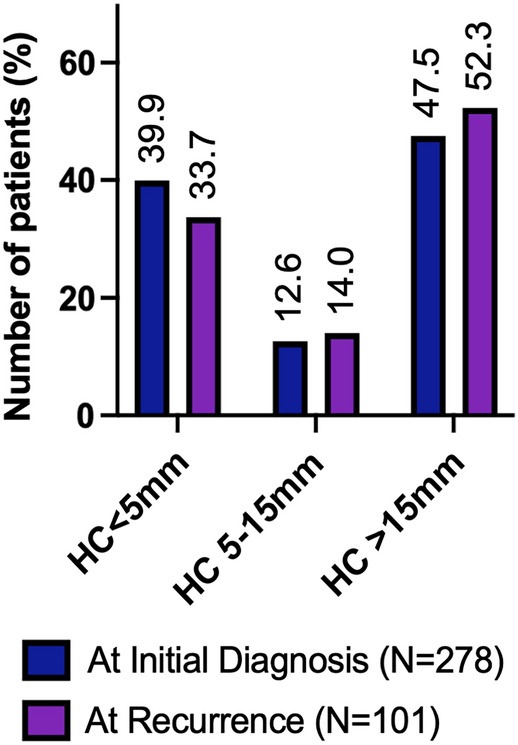
Results: Of the 278 patients diagnosed with PCNSL, 39.9% presented initial lesions at HAR. After induction therapy, 212 evaluable patients received consolidation treatments or observation. Intracranial failures occurred in 47.6% (n = 101), with 66.3% (n = 67) occurring outside the HAR and 33.7% (n = 34) inside the HAR. Unifocal disease (HR 0.61, 95% CI 0.39-0.96, p = 0.025) was associated with a lower risk of hippocampal failures, while initial HAR involvement significantly increased the risk (HR 2.26, 95% CI 1.18-4.47, p = 0.018). Patients with unifocal disease outside the HAR had the lowest 3-year hippocampal failure rate (6.2%). RT that included the hippocampus did not significantly affect hippocampal failure rates in patients without initial HAR lesions (p = 0.282), with three-year rates of 9.2 vs. 14.6% for other treatments. However, among patients with initial HAR involvement, RT including the hippocampus significantly reduced hippocampal failure rates compared to other approaches (p = 0.002). Hippocampal failure rates were comparable, with conventional WBRT at 14.6% and HA-WBRT at 19% in patients without initial HAR lesions (p = 0.734).
Conclusion: The routine application of the HA-WBRT strategy is not supported due to the high risk of hippocampal failures in general and requires further investigation to establish its feasibility and safety in well-defined subgroups. Our results suggest that the HA-WBRT strategy could be evaluated for select PCNSL patients with unifocal lesions or those located outside the HAR.
期刊介绍:
The Journal of Neuro-Oncology is a multi-disciplinary journal encompassing basic, applied, and clinical investigations in all research areas as they relate to cancer and the central nervous system. It provides a single forum for communication among neurologists, neurosurgeons, radiotherapists, medical oncologists, neuropathologists, neurodiagnosticians, and laboratory-based oncologists conducting relevant research. The Journal of Neuro-Oncology does not seek to isolate the field, but rather to focus the efforts of many disciplines in one publication through a format which pulls together these diverse interests. More than any other field of oncology, cancer of the central nervous system requires multi-disciplinary approaches. To alleviate having to scan dozens of journals of cell biology, pathology, laboratory and clinical endeavours, JNO is a periodical in which current, high-quality, relevant research in all aspects of neuro-oncology may be found.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
