Patrick Jacobsen Westphal, Cassiano Teixeira, João Ronaldo Mafalda Krauzer, Mirelle Hugo Bueno, Priscilla Alves Pereira, Sandro V Hostyn, Marcela Doebber Vieira, Camila Durante, Cristiane Bündchen
{"title":"Predictive factors for high-flow nasal cannula failure in patients with acute viral bronchiolitis admitted to the pediatric intensive care unit.","authors":"Patrick Jacobsen Westphal, Cassiano Teixeira, João Ronaldo Mafalda Krauzer, Mirelle Hugo Bueno, Priscilla Alves Pereira, Sandro V Hostyn, Marcela Doebber Vieira, Camila Durante, Cristiane Bündchen","doi":"10.62675/2965-2774.20250161","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To identify predictive factors for failure in the installation of high-flow nasal cannulas in children diagnosed with acute viral bronchiolitis under 24 months of age admitted to the pediatric intensive care unit.</p><p><strong>Methods: </strong>This work was a retrospective single-center cohort study conducted from March 2018 to July 2023 involving infants under 24 months of age who were diagnosed with acute viral bronchiolitis and who received high-flow nasal cannulas upon admission to the pediatric intensive care unit. Patients were categorized into two groups, the Success Group and Failure Group, on the basis of high-flow nasal cannula therapy efficacy. The primary outcome was treatment failure, which was defined as the transition to invasive or noninvasive ventilation. The analyzed variables included age, sex, weight, high-flow nasal cannula parameters, vital signs, risk factors, comorbidities, and imaging. Acute viral bronchiolitis severity was assessed using the Wood-Downes Scale, and functional status was assessed via the Functional Status Scale, both of which were administered by trained physiotherapists.</p><p><strong>Results: </strong>In total, 162 infants with acute viral bronchiolitis used high-flow nasal cannulas, with 17.28% experiencing treatment failure. The significant differences between the Failure and Success Groups included age (p = 0.001), weight (p = 0.002), bronchiolitis severity (p = 0.004), initial high-flow nasal cannula flow (p = 0.001), and duration of use (p = 0.000). The cutoff values for initial flow (≤ 12L/min), weight (≤ 5kg), and Wood-Downes score (≥ 9 points) were determined from the ROC curves. Initial flow ≤ 12L/min was the most predictive for failure (AUC = 0.71; 95%CI: 0.61 - 0.84; p = 0.001). Multivariate analysis indicated that weight was a protective factor (RR = 0.87; 95%CI: 0.78 - 0.98), duration of use reduced the risk of failure (RR = 0.49; 95%CI: 0.38 - 0.64; p = 0.000), and Wood-Downes score was not significant (RR = 1.04; 95%CI: 0.95 - 1.14; p = 0.427). Weight explained 84.7% of the variation in initial flow.</p><p><strong>Conclusion: </strong>Risk factors for high-flow nasal cannula therapy failure in bronchiolitis patients include younger age, consequently lower weight, and a lower initial flow rate.</p>","PeriodicalId":72721,"journal":{"name":"Critical care science","volume":"37 ","pages":"e20250161"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11869819/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.62675/2965-2774.20250161","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To identify predictive factors for failure in the installation of high-flow nasal cannulas in children diagnosed with acute viral bronchiolitis under 24 months of age admitted to the pediatric intensive care unit.
Methods: This work was a retrospective single-center cohort study conducted from March 2018 to July 2023 involving infants under 24 months of age who were diagnosed with acute viral bronchiolitis and who received high-flow nasal cannulas upon admission to the pediatric intensive care unit. Patients were categorized into two groups, the Success Group and Failure Group, on the basis of high-flow nasal cannula therapy efficacy. The primary outcome was treatment failure, which was defined as the transition to invasive or noninvasive ventilation. The analyzed variables included age, sex, weight, high-flow nasal cannula parameters, vital signs, risk factors, comorbidities, and imaging. Acute viral bronchiolitis severity was assessed using the Wood-Downes Scale, and functional status was assessed via the Functional Status Scale, both of which were administered by trained physiotherapists.
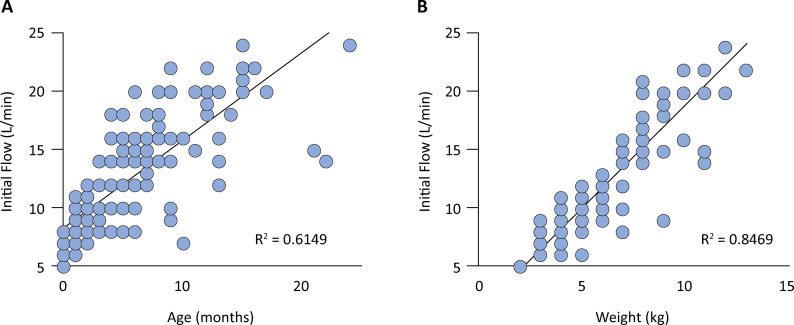
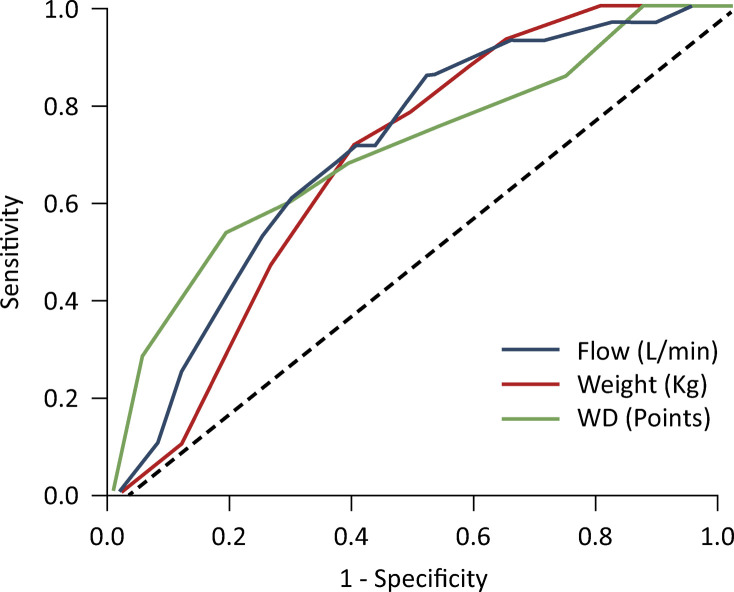
Results: In total, 162 infants with acute viral bronchiolitis used high-flow nasal cannulas, with 17.28% experiencing treatment failure. The significant differences between the Failure and Success Groups included age (p = 0.001), weight (p = 0.002), bronchiolitis severity (p = 0.004), initial high-flow nasal cannula flow (p = 0.001), and duration of use (p = 0.000). The cutoff values for initial flow (≤ 12L/min), weight (≤ 5kg), and Wood-Downes score (≥ 9 points) were determined from the ROC curves. Initial flow ≤ 12L/min was the most predictive for failure (AUC = 0.71; 95%CI: 0.61 - 0.84; p = 0.001). Multivariate analysis indicated that weight was a protective factor (RR = 0.87; 95%CI: 0.78 - 0.98), duration of use reduced the risk of failure (RR = 0.49; 95%CI: 0.38 - 0.64; p = 0.000), and Wood-Downes score was not significant (RR = 1.04; 95%CI: 0.95 - 1.14; p = 0.427). Weight explained 84.7% of the variation in initial flow.
Conclusion: Risk factors for high-flow nasal cannula therapy failure in bronchiolitis patients include younger age, consequently lower weight, and a lower initial flow rate.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
