Shawn Khan, Khushi Saigal, Jillene Moxam, Arash Maleki
{"title":"A Case of Concomitant Acute Zonal Occult Outer Retinopathy and Secondary Nonparaneoplastic Autoimmune Retinopathy.","authors":"Shawn Khan, Khushi Saigal, Jillene Moxam, Arash Maleki","doi":"10.1159/000543577","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute zonal occult outer retinopathy (AZOOR) is a rare inflammatory retinal disease with rapid outer retinal function loss, photopsias, unremarkable fundus findings, and electroretinography abnormalities. AZOOR diagnosis can be challenging due to its overlap with other retinal conditions, such as acute idiopathic blind spot enlargement syndrome and autoimmune retinopathies (AIRs). Multimodal imaging, including fundus autofluorescence and optical coherence tomography, has improved detection, revealing progressive outer retinal damage. Although the etiology of AZOOR remains uncertain, autoimmune mechanisms and viral associations have been proposed. Recent studies have identified anti-retinal antibodies, complicating differentiation from other AIRs.</p><p><strong>Case presentation: </strong>A 63-year-old male presented with photopsias, floaters, and worsening vision in his left eye. He had a prior diagnosis of AIR with serum antibodies against enolase, arrestin, and heat shock protein 27 (HSP27). Despite corticosteroid therapy, his visual acuity worsened from 20/20 to 20/60. Fundus examination showed subtle changes, and multimodal imaging revealed outer retinal damage consistent with AZOOR. He was started on mycophenolate mofetil, cyclosporine, and intravenous immunoglobulin. Over a year of follow-up, his vision improved to 20/25, and imaging showed stabilization of retinal damage.</p><p><strong>Conclusion: </strong>This case report highlights AZOOR can be associated with secondary np-AIR. Multimodal imaging, electrophysiologic testing of retina and retinal pigment epithelial, and anti-retinal antibody may be helpful for diagnosis of these patients. A combination of conventional immunomodulatory therapy and IVIg can help with controlling AZOOR and secondary np-AIR.</p>","PeriodicalId":9635,"journal":{"name":"Case Reports in Ophthalmology","volume":"16 1","pages":"124-132"},"PeriodicalIF":0.6000,"publicationDate":"2025-01-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842096/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543577","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Acute zonal occult outer retinopathy (AZOOR) is a rare inflammatory retinal disease with rapid outer retinal function loss, photopsias, unremarkable fundus findings, and electroretinography abnormalities. AZOOR diagnosis can be challenging due to its overlap with other retinal conditions, such as acute idiopathic blind spot enlargement syndrome and autoimmune retinopathies (AIRs). Multimodal imaging, including fundus autofluorescence and optical coherence tomography, has improved detection, revealing progressive outer retinal damage. Although the etiology of AZOOR remains uncertain, autoimmune mechanisms and viral associations have been proposed. Recent studies have identified anti-retinal antibodies, complicating differentiation from other AIRs.
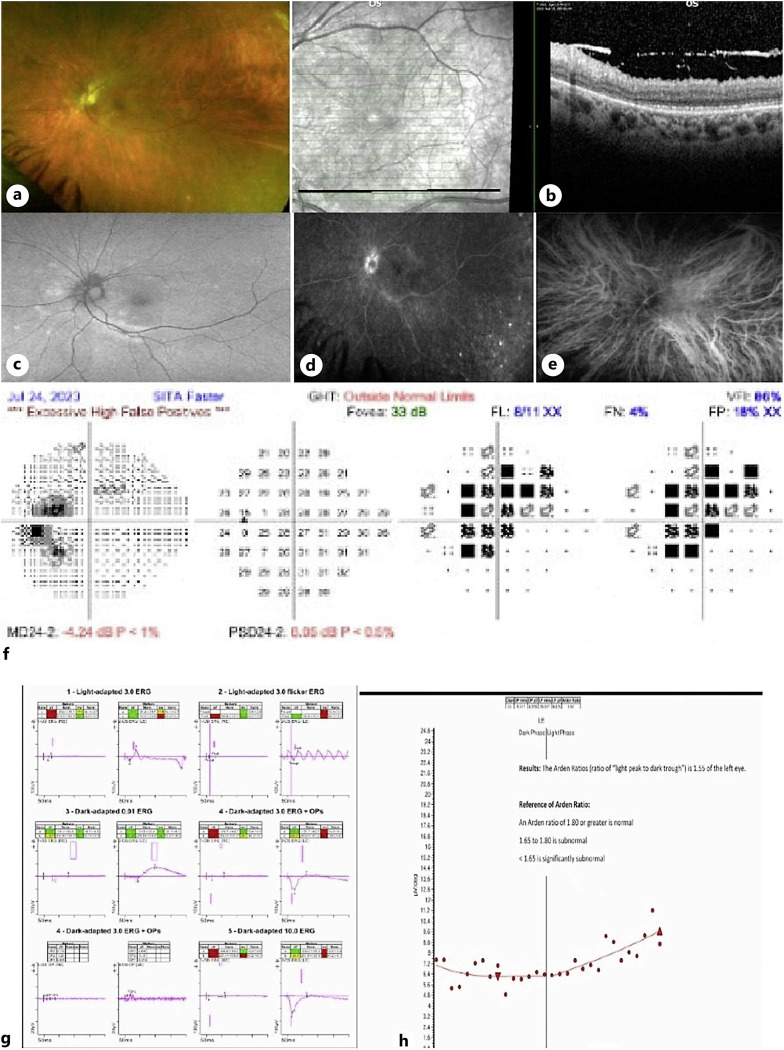
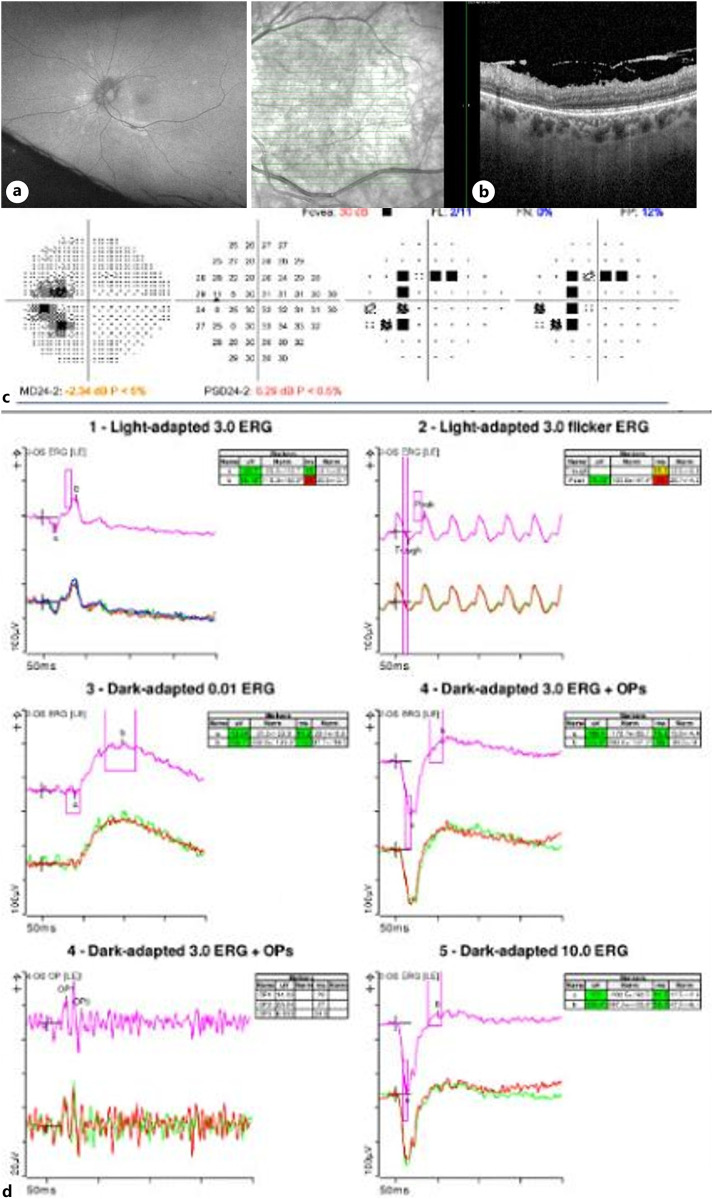
Case presentation: A 63-year-old male presented with photopsias, floaters, and worsening vision in his left eye. He had a prior diagnosis of AIR with serum antibodies against enolase, arrestin, and heat shock protein 27 (HSP27). Despite corticosteroid therapy, his visual acuity worsened from 20/20 to 20/60. Fundus examination showed subtle changes, and multimodal imaging revealed outer retinal damage consistent with AZOOR. He was started on mycophenolate mofetil, cyclosporine, and intravenous immunoglobulin. Over a year of follow-up, his vision improved to 20/25, and imaging showed stabilization of retinal damage.
Conclusion: This case report highlights AZOOR can be associated with secondary np-AIR. Multimodal imaging, electrophysiologic testing of retina and retinal pigment epithelial, and anti-retinal antibody may be helpful for diagnosis of these patients. A combination of conventional immunomodulatory therapy and IVIg can help with controlling AZOOR and secondary np-AIR.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of ophthalmology, including prevention, diagnosis, treatment, toxicities of therapy, supportive care, quality-of-life, and survivorship issues. The submission of negative results is strongly encouraged. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed. The intent of the journal is to provide clinicians and researchers with a tool to disseminate their personal experiences to a wider public as well as to review interesting cases encountered by colleagues all over the world. Universally used terms can be searched across the entire growing collection of case reports, further facilitating the retrieval of specific information. Following the open access principle, the entire contents can be retrieved at no charge, guaranteeing easy access to this valuable source of anecdotal information at all times.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
