{"title":"Economic Model of Uridine Triacetate Versus Supportive Care for the Treatment of Patients with Life-Threatening Early-Onset Severe Toxicity.","authors":"Jorge J Garcia, Alice Beers, Paige Reid, Salvatore Miragliotta, Suzanne Ward, Setareh A Williams, Michelle Barnard, Megan Bourque, Chantal Trepanier, Amanda Griffin","doi":"10.1007/s40261-025-01426-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Early-onset severe toxicity following the administration of 5-fluorouracil (5-FU) or capecitabine occurs in approximately 10-30% of patients receiving fluoropyrimidine therapy in the USA and is fatal to at least 0.5% of patients treated. Supportive care measures used to manage symptoms of toxicity are associated with extended hospital length of stay, high cost of care, and poor survival. Uridine triacetate is indicated as an emergency treatment for patients who exhibit early-onset, severe or life-threatening toxicity, and has been shown to significantly improve clinical outcomes. Despite its life-saving capability to reverse early-onset severe toxicity, uridine triacetate may be underutilized.</p><p><strong>Purpose: </strong>This study aims to evaluate the economic impact of uridine triacetate as a rescue therapy for adult patients from the US hospital payer perspective for early-onset severe toxicity, who are expected to die without treatment.</p><p><strong>Methods: </strong>A decision tree model was developed to compare inpatient survival, hospital length of stay, and inpatient healthcare resource utilization for patients treated with and without uridine triacetate. Costs associated with hospitalization, including supportive care measures and monitoring were evaluated, considering medications and procedures commonly used to manage various severe toxicities experienced (e.g., gastrointestinal, hematological, etc.). The model compared the hypothetical current practice, in which approximately half of patients expected to die from early-onset severe toxicity receive uridine triacetate in addition to supportive care, with the proposed future practice in which all eligible patients receive uridine triacetate during their hospital stay. Hypothetical practical scenarios for US institutions were also considered.</p><p><strong>Results: </strong>For each adult patient hospitalized for early-onset severe or life-threatening toxicity who would be expected to die without treatment, adoption of uridine triacetate as a rescue treatment was associated with clinical benefits, including increased inpatient survival (48.5%) and a 7.3-day reduction in total hospital length of stay per patient. Treatment of each additional patient with uridine triacetate was associated with an incremental cost of US$25,247 per patient. Seventy percent of the drug cost was offset by reduction in inpatient healthcare resources utilization. This cost offset is likely underestimated as it does not include additional savings from potential reimbursements associated with changes in hospital length of stay, readmissions and discounting. Hypothetical scenarios demonstrated that model outputs were most sensitive to changes in length of stay and hospitalization costs.</p><p><strong>Conclusion: </strong>Optimal treatment with uridine triacetate for all hospitalized patients in the USA expected to die from early-onset severe toxicity has the potential to improve inpatient survival at a minimal inpatient budget increase. The majority of the drug cost is offset by a reduction in the length of hospital stay and associated costs.</p>","PeriodicalId":10402,"journal":{"name":"Clinical Drug Investigation","volume":" ","pages":"111-123"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11876218/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Drug Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40261-025-01426-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
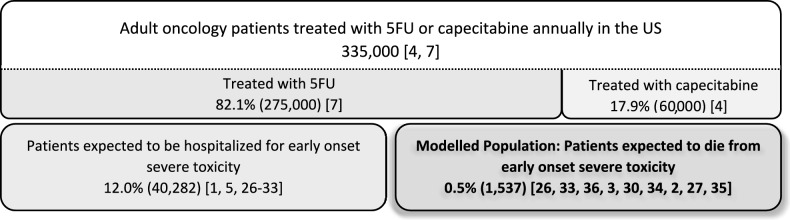
Background: Early-onset severe toxicity following the administration of 5-fluorouracil (5-FU) or capecitabine occurs in approximately 10-30% of patients receiving fluoropyrimidine therapy in the USA and is fatal to at least 0.5% of patients treated. Supportive care measures used to manage symptoms of toxicity are associated with extended hospital length of stay, high cost of care, and poor survival. Uridine triacetate is indicated as an emergency treatment for patients who exhibit early-onset, severe or life-threatening toxicity, and has been shown to significantly improve clinical outcomes. Despite its life-saving capability to reverse early-onset severe toxicity, uridine triacetate may be underutilized.
Purpose: This study aims to evaluate the economic impact of uridine triacetate as a rescue therapy for adult patients from the US hospital payer perspective for early-onset severe toxicity, who are expected to die without treatment.
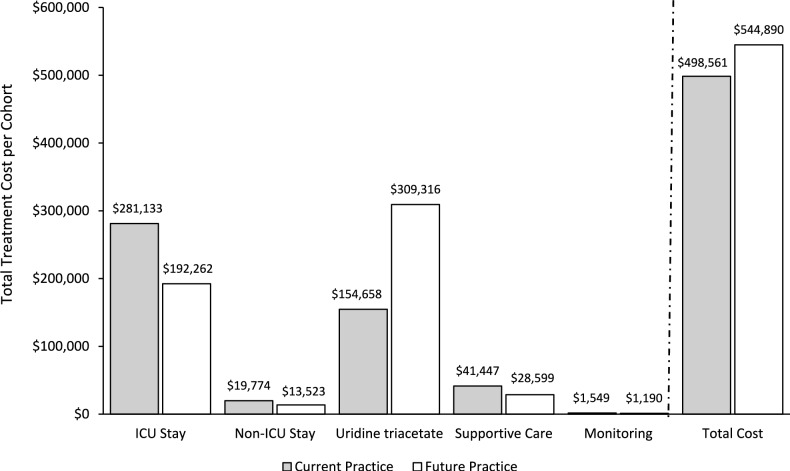
Methods: A decision tree model was developed to compare inpatient survival, hospital length of stay, and inpatient healthcare resource utilization for patients treated with and without uridine triacetate. Costs associated with hospitalization, including supportive care measures and monitoring were evaluated, considering medications and procedures commonly used to manage various severe toxicities experienced (e.g., gastrointestinal, hematological, etc.). The model compared the hypothetical current practice, in which approximately half of patients expected to die from early-onset severe toxicity receive uridine triacetate in addition to supportive care, with the proposed future practice in which all eligible patients receive uridine triacetate during their hospital stay. Hypothetical practical scenarios for US institutions were also considered.
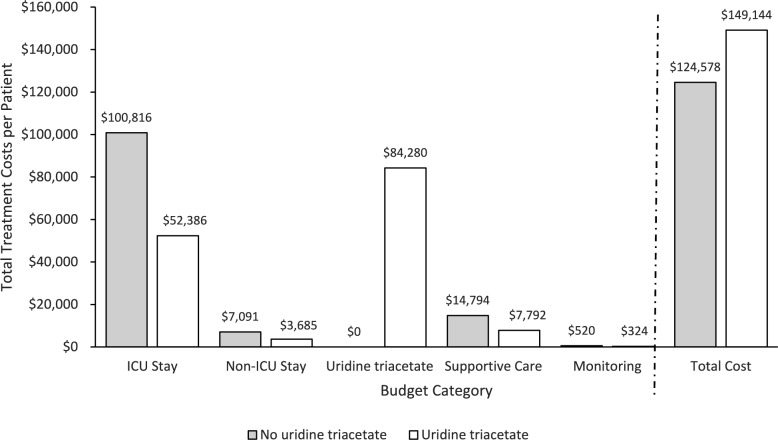
Results: For each adult patient hospitalized for early-onset severe or life-threatening toxicity who would be expected to die without treatment, adoption of uridine triacetate as a rescue treatment was associated with clinical benefits, including increased inpatient survival (48.5%) and a 7.3-day reduction in total hospital length of stay per patient. Treatment of each additional patient with uridine triacetate was associated with an incremental cost of US$25,247 per patient. Seventy percent of the drug cost was offset by reduction in inpatient healthcare resources utilization. This cost offset is likely underestimated as it does not include additional savings from potential reimbursements associated with changes in hospital length of stay, readmissions and discounting. Hypothetical scenarios demonstrated that model outputs were most sensitive to changes in length of stay and hospitalization costs.
Conclusion: Optimal treatment with uridine triacetate for all hospitalized patients in the USA expected to die from early-onset severe toxicity has the potential to improve inpatient survival at a minimal inpatient budget increase. The majority of the drug cost is offset by a reduction in the length of hospital stay and associated costs.
期刊介绍:
Clinical Drug Investigation provides rapid publication of original research covering all phases of clinical drug development and therapeutic use of drugs. The Journal includes:
-Clinical trials, outcomes research, clinical pharmacoeconomic studies and pharmacoepidemiology studies with a strong link to optimum prescribing practice for a drug or group of drugs.
-Clinical pharmacodynamic and clinical pharmacokinetic studies with a strong link to clinical practice.
-Pharmacodynamic and pharmacokinetic studies in healthy volunteers in which significant implications for clinical prescribing are discussed.
-Studies focusing on the application of drug delivery technology in healthcare.
-Short communications and case study reports that meet the above criteria will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Clinical Drug Investigation may be accompanied by plain language summaries to assist readers who have some knowledge, but non in-depth expertise in, the area to understand important medical advances.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
