{"title":"Genomic Profiling of Extensive Stage Small-Cell Lung Cancer Patients Identifies Molecular Factors Associated with Survival.","authors":"Matteo Canale, Milena Urbini, Elisabetta Petracci, Davide Angeli, Gianluca Tedaldi, Ilaria Priano, Paola Cravero, Michele Flospergher, Kalliopi Andrikou, Chiara Bennati, Davide Tassinari, Alessandra Dubini, Giulio Rossi, Riccardo Panzacchi, Mirca Valli, Giuseppe Bronte, Lucio Crinò, Angelo Delmonte, Paola Ulivi","doi":"10.2147/LCTT.S492825","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Extensive stage Small-Cell Lung Cancer (ES-SCLC) is the most lethal lung cancer, and the addition of immunotherapy conferred a slight survival benefit for patients. Extensive molecular profiling of patients treated with chemotherapy (CT) or chemotherapy plus immunotherapy (CT+IO) would be able to identify molecular factors associated with patients' survival.</p><p><strong>Material and methods: </strong>In this retrospective study, 99 ES-SCLC patients were considered. Of the 79 includible patients, 42 received CT (median age 71 y/o, I-IIIQ: 65-76), and 37 received CT+IO (median age 71 y/o, I-IIIQ 66-75). The FoundationOne CDx assay was performed on patients' tumor tissues.</p><p><strong>Results: </strong>The most mutated genes were <i>TP53</i> (99%), <i>RB1</i> (78%), <i>PTEN</i> (23%) and <i>MLL2</i> (20%), with no significant differences between the treatment groups. As a continuous variable, Tumor Mutation Burden (TMB) had an effect on patients' progression-free survival (PFS) by type of treatment (HR 1.81 (95%, CI: 0.99-3.31) and HR 0.84 (95%, CI: 0.56-1.26) for patients treated with CT and CT+IO, respectively). TMB was also computed and dichotomized using two different cut-offs: considering cut-offs of 10 mut/Mb and >16 mut/Mb, 45 patients (57%) and 68 patients (86.1%) had a low TMB, respectively. A high TMB (cut-off 10 mut/Mb) predicted worse PFS in patients treated with CT (<i>p</i>=0.046); even though not statistically significant, a high TMB (cut-off 16 mut/Mb) predicted a better survival in patients treated with CT+IO. Moreover, at univariate analysis, <i>MLL2</i> mutations were associated with better prognosis in the overall case series (HR<sub>PFS</sub> = 0.51, 95% CI: 0.28-0.94), and overall survival (HR<sub>OS</sub> = 0.52, 95% CI: 0.28-0.97).</p><p><strong>Conclusion: </strong>In ES-SCLC, TMB is associated with worse survival in patients treated with CT alone, and with better survival in patients treated with CT+IO, whether considered as a continuous or a dichotomized variable, at different cut-offs. Alterations in epigenetic factors are also associated to better patient prognosis.</p>","PeriodicalId":18066,"journal":{"name":"Lung Cancer: Targets and Therapy","volume":"16 ","pages":"11-23"},"PeriodicalIF":3.3000,"publicationDate":"2025-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11849429/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lung Cancer: Targets and Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LCTT.S492825","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Extensive stage Small-Cell Lung Cancer (ES-SCLC) is the most lethal lung cancer, and the addition of immunotherapy conferred a slight survival benefit for patients. Extensive molecular profiling of patients treated with chemotherapy (CT) or chemotherapy plus immunotherapy (CT+IO) would be able to identify molecular factors associated with patients' survival.
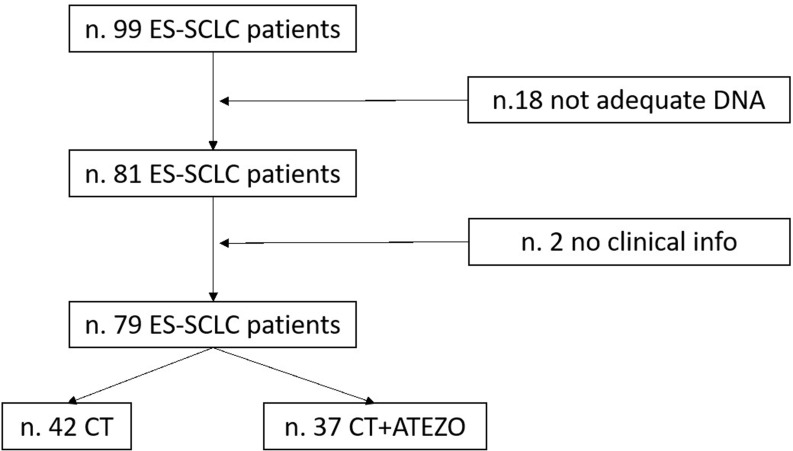
Material and methods: In this retrospective study, 99 ES-SCLC patients were considered. Of the 79 includible patients, 42 received CT (median age 71 y/o, I-IIIQ: 65-76), and 37 received CT+IO (median age 71 y/o, I-IIIQ 66-75). The FoundationOne CDx assay was performed on patients' tumor tissues.
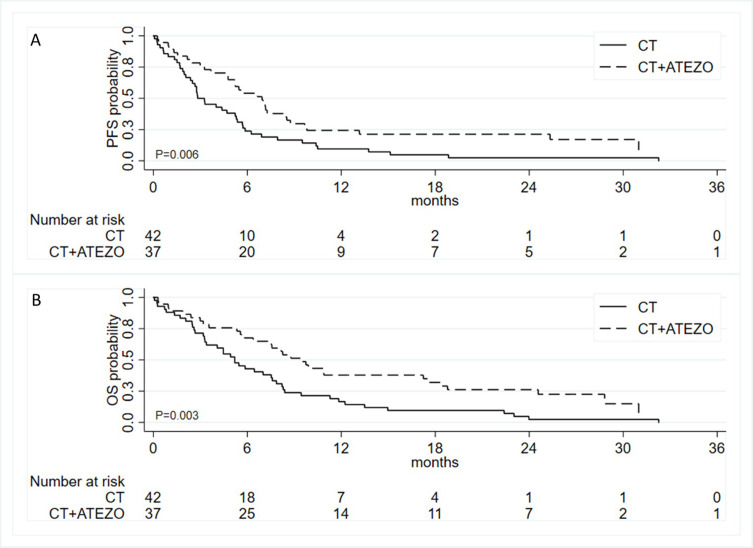
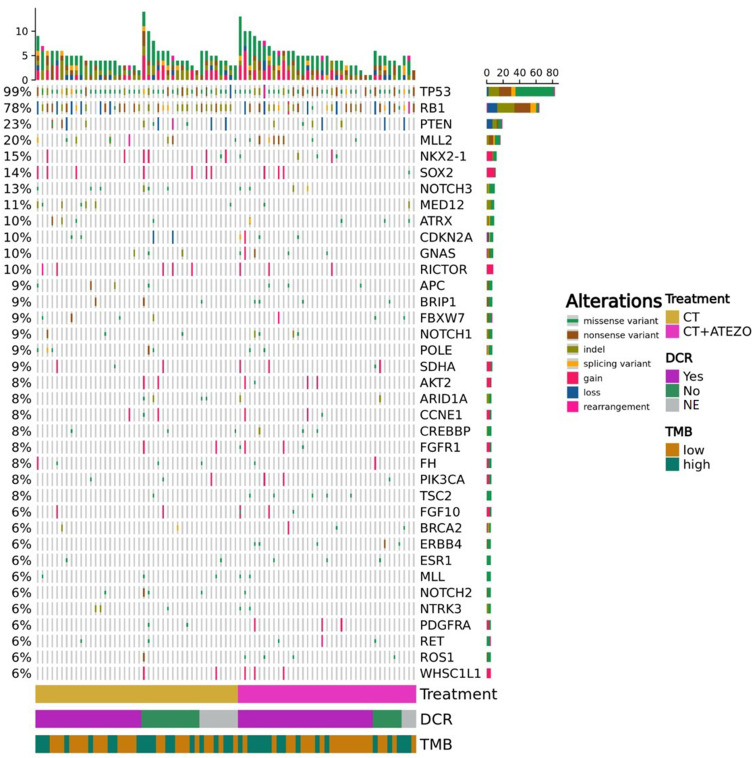
Results: The most mutated genes were TP53 (99%), RB1 (78%), PTEN (23%) and MLL2 (20%), with no significant differences between the treatment groups. As a continuous variable, Tumor Mutation Burden (TMB) had an effect on patients' progression-free survival (PFS) by type of treatment (HR 1.81 (95%, CI: 0.99-3.31) and HR 0.84 (95%, CI: 0.56-1.26) for patients treated with CT and CT+IO, respectively). TMB was also computed and dichotomized using two different cut-offs: considering cut-offs of 10 mut/Mb and >16 mut/Mb, 45 patients (57%) and 68 patients (86.1%) had a low TMB, respectively. A high TMB (cut-off 10 mut/Mb) predicted worse PFS in patients treated with CT (p=0.046); even though not statistically significant, a high TMB (cut-off 16 mut/Mb) predicted a better survival in patients treated with CT+IO. Moreover, at univariate analysis, MLL2 mutations were associated with better prognosis in the overall case series (HRPFS = 0.51, 95% CI: 0.28-0.94), and overall survival (HROS = 0.52, 95% CI: 0.28-0.97).
Conclusion: In ES-SCLC, TMB is associated with worse survival in patients treated with CT alone, and with better survival in patients treated with CT+IO, whether considered as a continuous or a dichotomized variable, at different cut-offs. Alterations in epigenetic factors are also associated to better patient prognosis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
