Emily R Wener, Sharon L Cushing, Blake C Papsin, Dimitrios J Stavropoulos, Roberto Mendoza-Londono, Nada Quercia, Karen A Gordon
{"title":"The Importance of Newborn Genetic Screening for Early Identification of GJB2 and SLC26A4 Related Hearing Loss.","authors":"Emily R Wener, Sharon L Cushing, Blake C Papsin, Dimitrios J Stavropoulos, Roberto Mendoza-Londono, Nada Quercia, Karen A Gordon","doi":"10.1002/ohn.1188","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess the added benefit of newborn genetic screening for GJB2 and SLC26A4 variants in conjunction with newborn hearing screening.</p><p><strong>Study design: </strong>Retrospective cohort study.</p><p><strong>Methods: </strong>Children with known variants of GJB2 and SLC26A4 were identified from 485 children with hearing loss who underwent testing with Next Generation Sequencing (NGS) between January 2015 and February 2018, prior to expanded screening for genetic variants and congenital CMV. Children with two pathogenic or likely pathogenic variants of GJB2 or SLC26A4 were considered to have genetic hearing loss. NGS genetic data were compared to variants included in the expanded genetic screen for all newborns in Ontario and newborn hearing screening results.</p><p><strong>Setting: </strong>Canadian tertiary pediatric hospital.</p><p><strong>Results: </strong>Thirty-five children with GJB2 and SLC26A4-associated hearing loss were identified by NGS (n = 27 GJB2-HL; n = 8 SLC26A4-HL). Of these, 20 (57%) had been identified by newborn hearing screening (14/27 52% GJB2-HL; 6/8 75% SLC26A4-HL). Ten of the 20 (50%) would also have been identified by genetic screening if it had been available (9/14 64% GJB2-HL; 1/6 17% SLC26A4-HL). An additional 8 children with GJB2 or SLC26A4-associated hearing loss passed their newborn hearing screen but showed hearing loss later; three of these children (38%) would have been identified by newborn genetic screening (3/6 GJB2-HL; 0/2 SLC26A4-HL).</p><p><strong>Conclusion: </strong>Genetic and hearing screening modalities in Ontario's expanded newborn hearing screening program improve early identification of children with hearing loss including those at risk of being missed by hearing screening alone. This was most clear for children with GJB2-hearing loss.</p>","PeriodicalId":19707,"journal":{"name":"Otolaryngology- Head and Neck Surgery","volume":" ","pages":"2082-2089"},"PeriodicalIF":2.5000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12120052/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Otolaryngology- Head and Neck Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ohn.1188","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/26 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To assess the added benefit of newborn genetic screening for GJB2 and SLC26A4 variants in conjunction with newborn hearing screening.
Study design: Retrospective cohort study.
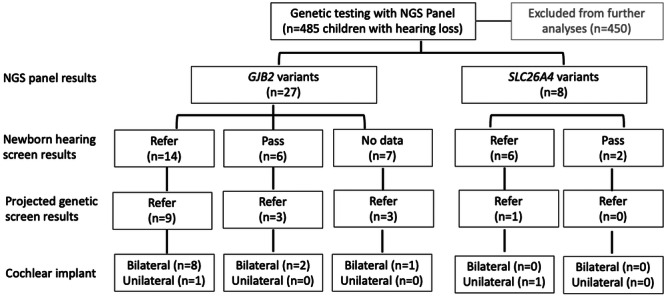
Methods: Children with known variants of GJB2 and SLC26A4 were identified from 485 children with hearing loss who underwent testing with Next Generation Sequencing (NGS) between January 2015 and February 2018, prior to expanded screening for genetic variants and congenital CMV. Children with two pathogenic or likely pathogenic variants of GJB2 or SLC26A4 were considered to have genetic hearing loss. NGS genetic data were compared to variants included in the expanded genetic screen for all newborns in Ontario and newborn hearing screening results.
Setting: Canadian tertiary pediatric hospital.
Results: Thirty-five children with GJB2 and SLC26A4-associated hearing loss were identified by NGS (n = 27 GJB2-HL; n = 8 SLC26A4-HL). Of these, 20 (57%) had been identified by newborn hearing screening (14/27 52% GJB2-HL; 6/8 75% SLC26A4-HL). Ten of the 20 (50%) would also have been identified by genetic screening if it had been available (9/14 64% GJB2-HL; 1/6 17% SLC26A4-HL). An additional 8 children with GJB2 or SLC26A4-associated hearing loss passed their newborn hearing screen but showed hearing loss later; three of these children (38%) would have been identified by newborn genetic screening (3/6 GJB2-HL; 0/2 SLC26A4-HL).
Conclusion: Genetic and hearing screening modalities in Ontario's expanded newborn hearing screening program improve early identification of children with hearing loss including those at risk of being missed by hearing screening alone. This was most clear for children with GJB2-hearing loss.
期刊介绍:
Otolaryngology–Head and Neck Surgery (OTO-HNS) is the official peer-reviewed publication of the American Academy of Otolaryngology–Head and Neck Surgery Foundation. The mission of Otolaryngology–Head and Neck Surgery is to publish contemporary, ethical, clinically relevant information in otolaryngology, head and neck surgery (ear, nose, throat, head, and neck disorders) that can be used by otolaryngologists, clinicians, scientists, and specialists to improve patient care and public health.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
