{"title":"Cognitive Authority Theory: Reframing health inequity, disadvantage and privilege in palliative and end-of-life care.","authors":"Katherine J Hunt, Carl R May","doi":"10.1177/02692163251321713","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There persist disparities in access to quality palliative and end-of-life care, often based on avoidable injustice. Research and theory to explain this health inequity focuses on structural or individual-based factors, overlooking important relational factors between health professionals, patients and families.</p><p><strong>Aim: </strong>To apply Cognitive Authority Theory in palliative and end-of-life care to explain neglected relational drivers of inequity in access and experience.</p><p><strong>Methods: </strong>Cognitive Authority Theory, a middle-range theory of power relations between individuals and authority over knowledge, was developed from empirical and review data. This paper demonstrates its utility in explaining an overlooked component of inequity in palliative care: interactions between health professionals and patients/caregivers.</p><p><strong>Results: </strong>Using examples from the palliative care literature, we characterise how people who are socially disadvantaged have fewer resources to exploit during consultations with health professionals which makes it difficult for them to have their voices heard, their choices prioritised by others, and to express their expertise. We examine the implications of health professionals' judgements of expertise for care access, experience, involvement and appropriateness. We offer a fresh perspective on the mechanisms by which stereotypes, bias and power imbalances between health professionals and patients reinforce existing health inequities, drawing on the role of social privilege in shaping inequity in palliative care.</p><p><strong>Conclusion: </strong>This paper provides a new language to articulate relational drivers of inequity in palliative care. It explains how to use Cognitive Authority Theory to design and interpret research to determine how healthcare interactions reinforce both social privilege and social disadvantage at end-of-life.</p>","PeriodicalId":19849,"journal":{"name":"Palliative Medicine","volume":" ","pages":"448-459"},"PeriodicalIF":3.9000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11977813/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/02692163251321713","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/26 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There persist disparities in access to quality palliative and end-of-life care, often based on avoidable injustice. Research and theory to explain this health inequity focuses on structural or individual-based factors, overlooking important relational factors between health professionals, patients and families.
Aim: To apply Cognitive Authority Theory in palliative and end-of-life care to explain neglected relational drivers of inequity in access and experience.
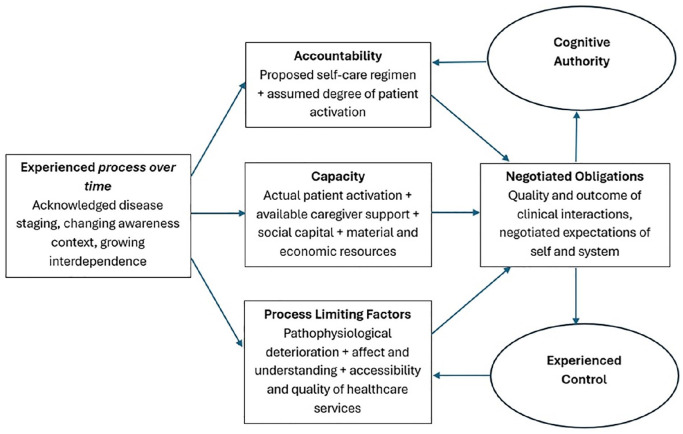
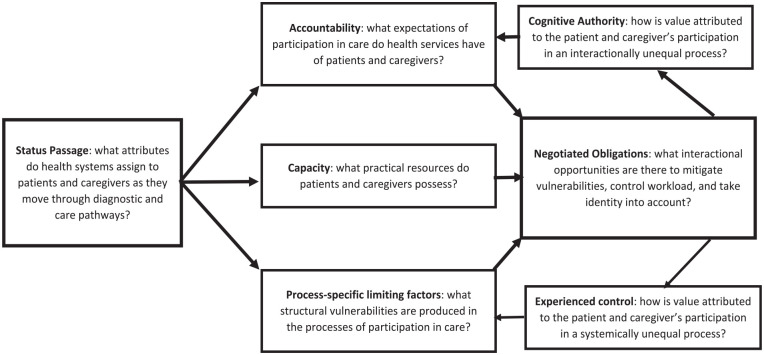
Methods: Cognitive Authority Theory, a middle-range theory of power relations between individuals and authority over knowledge, was developed from empirical and review data. This paper demonstrates its utility in explaining an overlooked component of inequity in palliative care: interactions between health professionals and patients/caregivers.
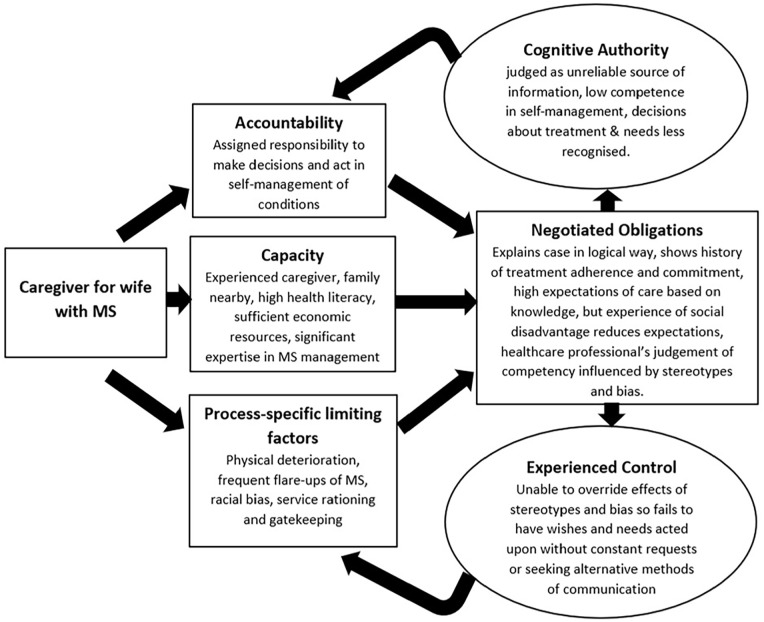
Results: Using examples from the palliative care literature, we characterise how people who are socially disadvantaged have fewer resources to exploit during consultations with health professionals which makes it difficult for them to have their voices heard, their choices prioritised by others, and to express their expertise. We examine the implications of health professionals' judgements of expertise for care access, experience, involvement and appropriateness. We offer a fresh perspective on the mechanisms by which stereotypes, bias and power imbalances between health professionals and patients reinforce existing health inequities, drawing on the role of social privilege in shaping inequity in palliative care.
Conclusion: This paper provides a new language to articulate relational drivers of inequity in palliative care. It explains how to use Cognitive Authority Theory to design and interpret research to determine how healthcare interactions reinforce both social privilege and social disadvantage at end-of-life.
期刊介绍:
Palliative Medicine is a highly ranked, peer reviewed scholarly journal dedicated to improving knowledge and clinical practice in the palliative care of patients with far advanced disease. This outstanding journal features editorials, original papers, review articles, case reports, correspondence and book reviews. Essential reading for all members of the palliative care team. This journal is a member of the Committee on Publication Ethics (COPE).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
