Mazen Zamzam, Colin Van Wagoner, Imran Bitar, Ehab Saleh
{"title":"Pediatric Rupture of Hallux Interphalangeal Joint Lateral Collateral Ligament.","authors":"Mazen Zamzam, Colin Van Wagoner, Imran Bitar, Ehab Saleh","doi":"10.5435/JAAOSGlobal-D-24-00307","DOIUrl":null,"url":null,"abstract":"<p><p>Ligamentous injuries of the hallux are rare, and when seen, they are most commonly treated conservatively. Surgical treatment of such injuries is also rare, making reports on the postoperative outcome and complications even less frequent. A case report of a hallux interphalangeal joint (IPJ) lateral collateral ligament tear in a 16-year-old gymnast is presented. Initially, she presented to the clinic with pain in her left hallux. She injured her toe while doing a gymnastic maneuver in which it got stuck and hyperextended. Physical examination revealed pain in her left great toe metatarsophalangeal and IPJs. Her medical history included the diagnosis of Ehlers-Danlos syndrome. She was managed conservatively with a controlled ankle motion boot for 4 weeks. When she returned for follow-up, her physical examination showed increased laxity to the great toe IPJ lateral collateral ligament compared with the other foot. A left foot MRI was done, which showed a complete rupture of the IPJ lateral collateral ligament origin (Figure 1). She underwent surgical intervention 6 weeks following her injury, in which the collateral ligament was repaired with suture anchors along with IP joint pinning to protect the repair (Figure 2). Following surgery, she returned to the clinic because of persistent drainage from a small hole near the incision site. During further incision and débridement, we discovered granulomatous tissue surrounding an embedded suture. The suture was removed, and the wound was irrigated. Following this procedure, the patient recovered fully in 3 weeks. She was provided a home exercise program and returned to gymnastics without limitations, toe pain, or instability. This case demonstrates an interesting complication following collateral ligament repair in the hallux.</p>","PeriodicalId":45062,"journal":{"name":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","volume":"9 3","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11878989/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Academy of Orthopaedic Surgeons Global Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5435/JAAOSGlobal-D-24-00307","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
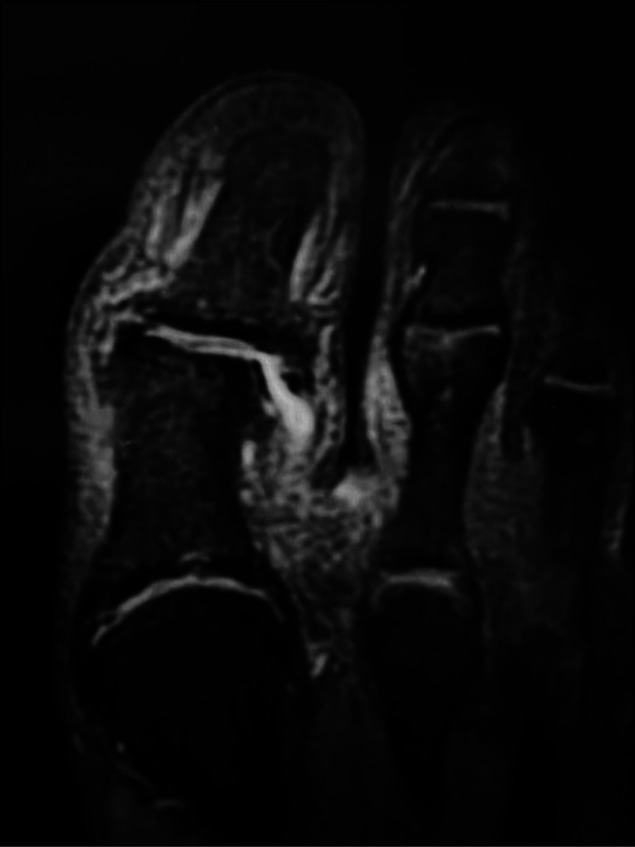
Ligamentous injuries of the hallux are rare, and when seen, they are most commonly treated conservatively. Surgical treatment of such injuries is also rare, making reports on the postoperative outcome and complications even less frequent. A case report of a hallux interphalangeal joint (IPJ) lateral collateral ligament tear in a 16-year-old gymnast is presented. Initially, she presented to the clinic with pain in her left hallux. She injured her toe while doing a gymnastic maneuver in which it got stuck and hyperextended. Physical examination revealed pain in her left great toe metatarsophalangeal and IPJs. Her medical history included the diagnosis of Ehlers-Danlos syndrome. She was managed conservatively with a controlled ankle motion boot for 4 weeks. When she returned for follow-up, her physical examination showed increased laxity to the great toe IPJ lateral collateral ligament compared with the other foot. A left foot MRI was done, which showed a complete rupture of the IPJ lateral collateral ligament origin (Figure 1). She underwent surgical intervention 6 weeks following her injury, in which the collateral ligament was repaired with suture anchors along with IP joint pinning to protect the repair (Figure 2). Following surgery, she returned to the clinic because of persistent drainage from a small hole near the incision site. During further incision and débridement, we discovered granulomatous tissue surrounding an embedded suture. The suture was removed, and the wound was irrigated. Following this procedure, the patient recovered fully in 3 weeks. She was provided a home exercise program and returned to gymnastics without limitations, toe pain, or instability. This case demonstrates an interesting complication following collateral ligament repair in the hallux.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
