{"title":"Incremental value of physiological indices to predict high-risk plaques detected by NIRS-IVUS.","authors":"Kazuyoshi Kakehi, Masafumi Ueno, Nobuhiro Yamada, Kyohei Onishi, Keishiro Sugimoto, Yohei Funauchi, Takayuki Kawamura, Kosuke Fujita, Hiroki Matsuzoe, Koichiro Matsumura, Gaku Nakazawa","doi":"10.1007/s12928-025-01116-7","DOIUrl":null,"url":null,"abstract":"<p><p>Identification of vulnerable plaques is important for reducing future cardiovascular events. This study aimed to investigate optimal modalities other than intravascular imaging in evaluating vulnerable plaques. We prospectively evaluated 105 non-culprit coronary lesions by CCTA imaging and near-infrared spectroscopy-intravascular ultrasound in 32 patients with acute coronary syndrome. Angiographically-derived ΔQFR and ΔFFR<sub>CT</sub> were measured as the difference in QFR and FFR<sub>CT</sub> across the stenosis. A receiver operating characteristic curve analysis was performed to determine the optimal cutoff values of angiographically- and CCTA-derived plaque features for a maxLCBI<sub>4mm</sub> ≥ 400. The best cutoff values for ΔQFR and ΔFFR<sub>CT</sub> to predict a maxLCBI<sub>4mm</sub> ≥ 400 were 0.05 and 0.06, respectively. ΔQFR and ΔFFR<sub>CT</sub> values and percent diameter stenosis on QCA or CCTA were associated with a maxLCBI<sub>4mm</sub> ≥ 400 (both P < 0.05). The combination of ΔFFR<sub>CT</sub> ≥ 0.06 and plaque density predicted a maxLCBI<sub>4mm</sub> ≥ 400 with 89.4% sensitivity and 84.5% specificity (area under the curve, 0.90; P < 0.0001). There was no significant difference in area under the curve values between ΔQFR and plaque density + ΔFFR<sub>CT</sub> ≥ 0.06 (0.92 vs. 0.90, P = 0.50). In the diagnosis of vulnerable plaques in acute coronary syndrome, the combination of ΔFFR<sub>CT</sub> and plaque density shows a diagnostic capability similar to that of ΔQFR in non-culprit lesions.</p>","PeriodicalId":9439,"journal":{"name":"Cardiovascular Intervention and Therapeutics","volume":" ","pages":"588-598"},"PeriodicalIF":5.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167347/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Intervention and Therapeutics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12928-025-01116-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
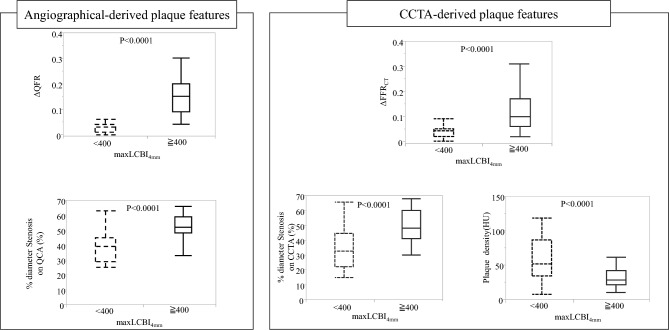
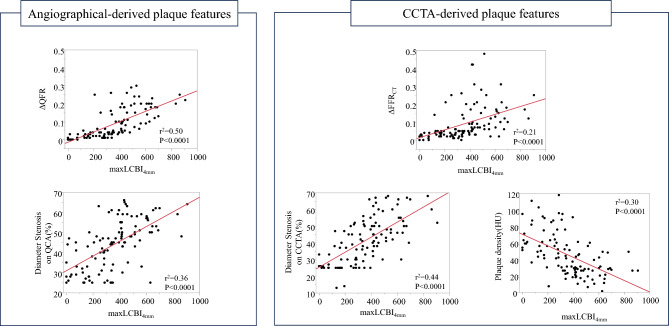
Identification of vulnerable plaques is important for reducing future cardiovascular events. This study aimed to investigate optimal modalities other than intravascular imaging in evaluating vulnerable plaques. We prospectively evaluated 105 non-culprit coronary lesions by CCTA imaging and near-infrared spectroscopy-intravascular ultrasound in 32 patients with acute coronary syndrome. Angiographically-derived ΔQFR and ΔFFRCT were measured as the difference in QFR and FFRCT across the stenosis. A receiver operating characteristic curve analysis was performed to determine the optimal cutoff values of angiographically- and CCTA-derived plaque features for a maxLCBI4mm ≥ 400. The best cutoff values for ΔQFR and ΔFFRCT to predict a maxLCBI4mm ≥ 400 were 0.05 and 0.06, respectively. ΔQFR and ΔFFRCT values and percent diameter stenosis on QCA or CCTA were associated with a maxLCBI4mm ≥ 400 (both P < 0.05). The combination of ΔFFRCT ≥ 0.06 and plaque density predicted a maxLCBI4mm ≥ 400 with 89.4% sensitivity and 84.5% specificity (area under the curve, 0.90; P < 0.0001). There was no significant difference in area under the curve values between ΔQFR and plaque density + ΔFFRCT ≥ 0.06 (0.92 vs. 0.90, P = 0.50). In the diagnosis of vulnerable plaques in acute coronary syndrome, the combination of ΔFFRCT and plaque density shows a diagnostic capability similar to that of ΔQFR in non-culprit lesions.
易损斑块的识别对于减少未来心血管事件非常重要。本研究旨在探讨除血管内成像外评估易损斑块的最佳方式。我们对32例急性冠状动脉综合征患者的105个非罪魁祸首冠状动脉病变进行了前瞻性的CCTA成像和近红外光谱血管内超声评估。血管造影衍生的ΔQFR和ΔFFRCT测量狭窄间QFR和FFRCT的差异。对maxLCBI4mm≥400的患者进行受试者工作特征曲线分析,以确定血管造影和ccta衍生斑块特征的最佳临界值。ΔQFR和ΔFFRCT预测maxLCBI4mm≥400的最佳截止值分别为0.05和0.06。ΔQFR和ΔFFRCT值以及QCA或CCTA上的直径狭窄百分比与maxLCBI4mm≥400相关(P CT均≥0.06,斑块密度预测maxLCBI4mm≥400具有89.4%的敏感性和84.5%的特异性(曲线下面积,0.90;P CT≥0.06 (0.92 vs. 0.90, P = 0.50)。在急性冠状动脉综合征易损斑块的诊断中,ΔFFRCT和斑块密度的结合与ΔQFR在非罪魁祸首病变中的诊断能力相似。
期刊介绍:
Cardiovascular Intervention and Therapeutics (CVIT) is an international journal covering the field of cardiovascular disease and includes cardiac (coronary and noncoronary) and peripheral interventions and therapeutics. Articles are subject to peer review and complete editorial evaluation prior to any decision regarding acceptability. CVIT is an official journal of The Japanese Association of Cardiovascular Intervention and Therapeutics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
