Accuracy evaluation of preoperative indocyanine green tattooing and intraoperative colonoscopy in determining surgical resection margins for left-sided colorectal cancer: a retrospective study in Korea.
Byung-Soo Park, Sung Hwan Cho, Gyung Mo Son, Hyun Sung Kim, Jin Ook Jang, Dae Gon Ryu, Su Jin Kim, Su Bum Park, Hyung Wook Kim
{"title":"Accuracy evaluation of preoperative indocyanine green tattooing and intraoperative colonoscopy in determining surgical resection margins for left-sided colorectal cancer: a retrospective study in Korea.","authors":"Byung-Soo Park, Sung Hwan Cho, Gyung Mo Son, Hyun Sung Kim, Jin Ook Jang, Dae Gon Ryu, Su Jin Kim, Su Bum Park, Hyung Wook Kim","doi":"10.7602/jmis.2025.28.1.19","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We aimed to evaluate the precision of preoperative colonoscopic tattooing and intraoperative colonoscopic tumor localization in determining distal surgical margins for left-sided colorectal cancer surgery.</p><p><strong>Methods: </strong>This retrospective study included 30 patients who underwent laparoscopic colorectal surgery, preoperative colonoscopic tattooing, and intraoperative colonoscopic localization for colorectal cancer at our center between July 2020 and March 2024. Clinical data were collected, and the precision of these methods was assessed by measuring the differences between the target resection margin and the actual pathological resection margin.</p><p><strong>Results: </strong>In four patient cases, the indocyanine green tattoo was not visible in the laparoscopic surgical field. The average stained length of the tattoo was 2.89 cm, with a mean distance of 1.18 cm between the low margin of the tattoo and the cancer. The difference between the target distal resection margin by intraoperative colonoscopic localization and the actual pathological resection margin was 0.88 cm. No complications related to the intraoperative colonoscopy were observed.</p><p><strong>Conclusion: </strong>Preoperative tattooing showed limitations, such as spreading and occasional invisibility. Intraoperative colonoscopic localization proved to be an effective method for achieving more precise distal surgical margins in left-sided colorectal cancer surgery.</p>","PeriodicalId":73832,"journal":{"name":"Journal of minimally invasive surgery","volume":"28 1","pages":"19-24"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11914831/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of minimally invasive surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7602/jmis.2025.28.1.19","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: We aimed to evaluate the precision of preoperative colonoscopic tattooing and intraoperative colonoscopic tumor localization in determining distal surgical margins for left-sided colorectal cancer surgery.
Methods: This retrospective study included 30 patients who underwent laparoscopic colorectal surgery, preoperative colonoscopic tattooing, and intraoperative colonoscopic localization for colorectal cancer at our center between July 2020 and March 2024. Clinical data were collected, and the precision of these methods was assessed by measuring the differences between the target resection margin and the actual pathological resection margin.
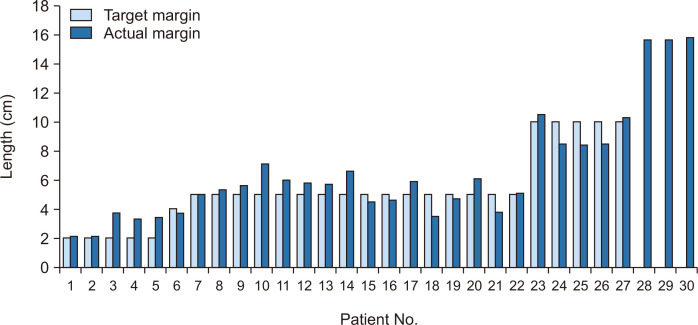
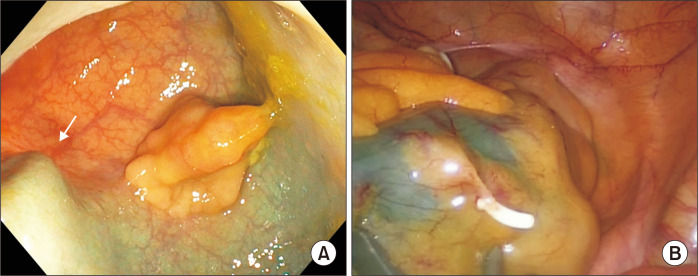
Results: In four patient cases, the indocyanine green tattoo was not visible in the laparoscopic surgical field. The average stained length of the tattoo was 2.89 cm, with a mean distance of 1.18 cm between the low margin of the tattoo and the cancer. The difference between the target distal resection margin by intraoperative colonoscopic localization and the actual pathological resection margin was 0.88 cm. No complications related to the intraoperative colonoscopy were observed.
Conclusion: Preoperative tattooing showed limitations, such as spreading and occasional invisibility. Intraoperative colonoscopic localization proved to be an effective method for achieving more precise distal surgical margins in left-sided colorectal cancer surgery.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
