{"title":"The Real-World Use of Semaglutide to Promote Weight Loss in Obese Adults With Hemodialysis: A Multicenter Cross-Sectional Descriptive Study.","authors":"Jodianne Couture, Pascale Robert, Marie-France Beauchesne, Gabriel Dallaire, Annie Lizotte, Jo-Annie Lafrenière, Julie Beauregard, Janique Doucet","doi":"10.1177/20543581251324588","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Obesity can be an issue for renal transplant eligibility. Semaglutide constitutes an interesting choice for obesity treatment, but little data exist regarding its efficacy and security among dialysis patients.</p><p><strong>Objectives: </strong>The co-primary endpoints of this study were to describe the change in body weight (%) and in body mass index (BMI) from the beginning and after 3, 6, and 12 months of treatment for participants who used semaglutide compared with a control group of non-users. Secondary endpoints included description of dosages used and reported adverse events.</p><p><strong>Design: </strong>Multicenter cross-sectional descriptive study.</p><p><strong>Setting: </strong>Seven hemodialysis centers in Quebec and New Brunswick, Canada.</p><p><strong>Patients: </strong>Adults receiving hemodialysis treatment with BMI of at least 30 kg/m<sup>2</sup> were included.</p><p><strong>Measurements: </strong>Weight as defined by the target body weight (kg) at the end of dialysis. Body mass index is defined by weight, kg/m<sup>2</sup>.</p><p><strong>Methods: </strong>As a primary objective, we collected in records the body weights and calculated BMI at months 0, 3, 6, and 12 for participants with BMI of 30 kg/m<sup>2</sup> or greater. The dosages of semaglutide and the mention of any adverse events were also collected from questionnaire to participants, to community drug stores, and from records.</p><p><strong>Results: </strong>A total of 1286 patients received hemodialysis treatments in June 2023. Of these, 396 (31%) had a BMI of 30 kg/m<sup>2</sup> or greater. Two hundred fifty-one participants were included in the study and 41 (16%) received semaglutide. The estimated treatment differences for the percentage change in body weight from baseline to 3, 6, and 12 months for semaglutide compared with the control group were -2.26%, 95% confidence interval (CI), -3.68 to -0.84, <i>P</i> = .002; -0.94%, 95% CI, -2.17 to 0.29, <i>P</i> = 0.135; and -0.64%; 95% CI, -2.04 to 0.76, <i>P</i> = .370, respectively. The estimated treatment differences at 3, 6, and 12 months for BMI were -0.87 kg/m<sup>2</sup>, 95% CI, -1.38 to -0.36, <i>P</i> < .001; -0.35 kg/m<sup>2</sup>, 95% CI, -0.79 to 0.09, <i>P</i> = .119; and -0.23 kg/m<sup>2</sup>, 95% CI, -0.72 to 0.27, <i>P</i> = .371, respectively. The estimated treatment difference in body weight and BMI change between the 2 groups was statistically significant at 3 months. A sensitivity analysis was carried out with all the participants of the semaglutide group who continued the treatment for 12 months (N = 15). The estimated treatment differences for the percentage change in body weight between this group and the control group were -3.04%, 95% CI, -5.18 to -0.89, <i>P</i> = .006; -1.97%, 95% CI, -3.79 to -0.14, <i>P</i> = .035; and -2.83%, 95% CI, -4.66 to -1.00, <i>P</i> = .003 at 3, 6, and 12 months, respectively. The average body weight change between months 0 and 12 was -3.88 ± 7.90 kg in the semaglutide group compared with -0.52 ± 5.53 kg in the control group (<i>P</i> = .015). With the sensitivity analysis, the body weight change between Months 0 and 12 was -6.83 ± 6.90 kg for the participants who continued their treatment for 12 months. The dosage of 1 mg of semaglutide was the most prescribed (49%). The occurrence of adverse events led to dose reduction in 5 participants (12%) and to treatment discontinuation in 13 participants (32%).</p><p><strong>Limitations: </strong>This study has several limitations, including its non-randomized design, short follow-up period, small sample size, and incomplete data on treatment compliance and adverse effects. Differences in patient characteristics, limited semaglutide doses for weight loss, and declining sample sizes over time further reduce the strength of conclusions, necessitating cautious interpretation of group comparisons.</p><p><strong>Conclusions: </strong>This study suggests that semaglutide promotes weight loss in hemodialyzed adults with obesity, but discontinuation of treatment was frequent and common adverse events were reported.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251324588"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915253/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251324588","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Obesity can be an issue for renal transplant eligibility. Semaglutide constitutes an interesting choice for obesity treatment, but little data exist regarding its efficacy and security among dialysis patients.
Objectives: The co-primary endpoints of this study were to describe the change in body weight (%) and in body mass index (BMI) from the beginning and after 3, 6, and 12 months of treatment for participants who used semaglutide compared with a control group of non-users. Secondary endpoints included description of dosages used and reported adverse events.
Setting: Seven hemodialysis centers in Quebec and New Brunswick, Canada.
Patients: Adults receiving hemodialysis treatment with BMI of at least 30 kg/m2 were included.
Measurements: Weight as defined by the target body weight (kg) at the end of dialysis. Body mass index is defined by weight, kg/m2.
Methods: As a primary objective, we collected in records the body weights and calculated BMI at months 0, 3, 6, and 12 for participants with BMI of 30 kg/m2 or greater. The dosages of semaglutide and the mention of any adverse events were also collected from questionnaire to participants, to community drug stores, and from records.
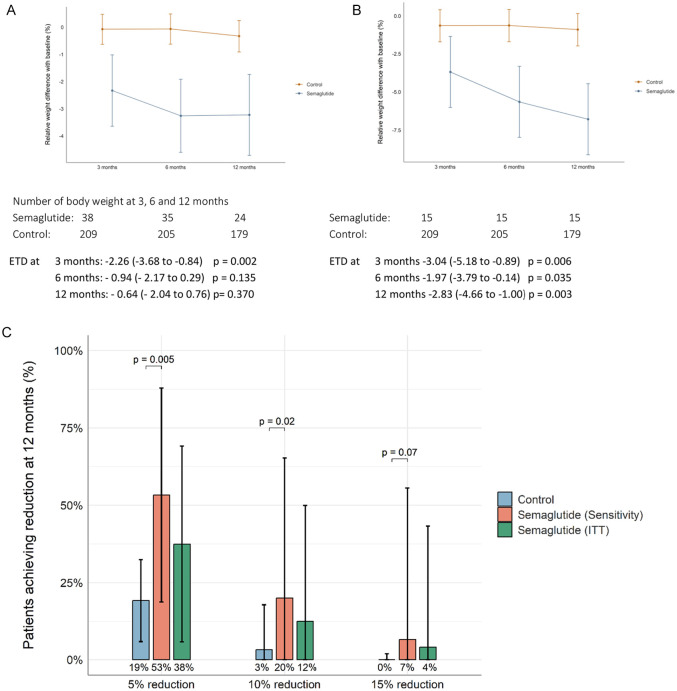
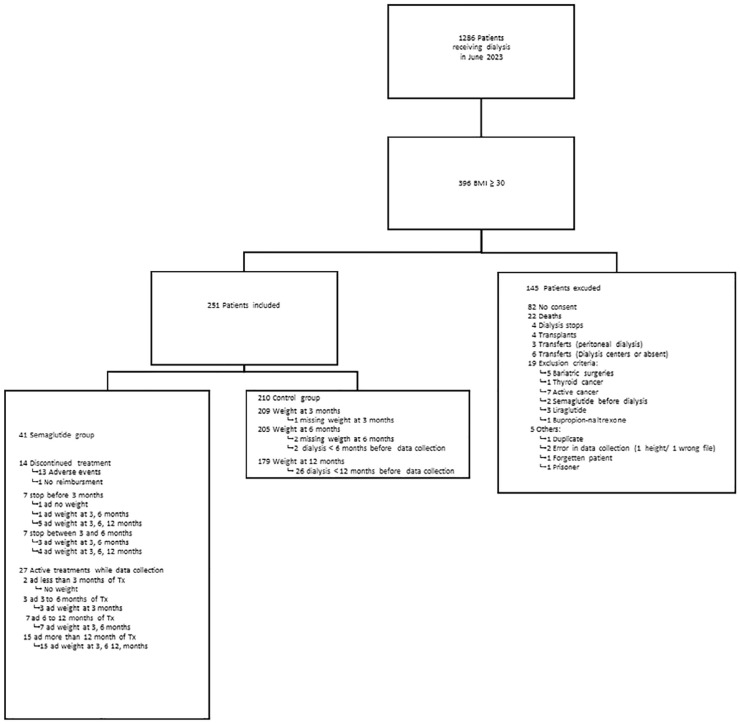
Results: A total of 1286 patients received hemodialysis treatments in June 2023. Of these, 396 (31%) had a BMI of 30 kg/m2 or greater. Two hundred fifty-one participants were included in the study and 41 (16%) received semaglutide. The estimated treatment differences for the percentage change in body weight from baseline to 3, 6, and 12 months for semaglutide compared with the control group were -2.26%, 95% confidence interval (CI), -3.68 to -0.84, P = .002; -0.94%, 95% CI, -2.17 to 0.29, P = 0.135; and -0.64%; 95% CI, -2.04 to 0.76, P = .370, respectively. The estimated treatment differences at 3, 6, and 12 months for BMI were -0.87 kg/m2, 95% CI, -1.38 to -0.36, P < .001; -0.35 kg/m2, 95% CI, -0.79 to 0.09, P = .119; and -0.23 kg/m2, 95% CI, -0.72 to 0.27, P = .371, respectively. The estimated treatment difference in body weight and BMI change between the 2 groups was statistically significant at 3 months. A sensitivity analysis was carried out with all the participants of the semaglutide group who continued the treatment for 12 months (N = 15). The estimated treatment differences for the percentage change in body weight between this group and the control group were -3.04%, 95% CI, -5.18 to -0.89, P = .006; -1.97%, 95% CI, -3.79 to -0.14, P = .035; and -2.83%, 95% CI, -4.66 to -1.00, P = .003 at 3, 6, and 12 months, respectively. The average body weight change between months 0 and 12 was -3.88 ± 7.90 kg in the semaglutide group compared with -0.52 ± 5.53 kg in the control group (P = .015). With the sensitivity analysis, the body weight change between Months 0 and 12 was -6.83 ± 6.90 kg for the participants who continued their treatment for 12 months. The dosage of 1 mg of semaglutide was the most prescribed (49%). The occurrence of adverse events led to dose reduction in 5 participants (12%) and to treatment discontinuation in 13 participants (32%).
Limitations: This study has several limitations, including its non-randomized design, short follow-up period, small sample size, and incomplete data on treatment compliance and adverse effects. Differences in patient characteristics, limited semaglutide doses for weight loss, and declining sample sizes over time further reduce the strength of conclusions, necessitating cautious interpretation of group comparisons.
Conclusions: This study suggests that semaglutide promotes weight loss in hemodialyzed adults with obesity, but discontinuation of treatment was frequent and common adverse events were reported.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
