{"title":"Pitfalls in diagnosis of atypical atrioventricular nodal reentrant tachycardia by a conventional electrophysiological study","authors":"Mihoko Kawabata MD , Yasuhiro Shirai MD , Tatsuaki Kamata MD , Tomoyuki Kawashima MD , Ryo Yonai MD , Kaoru Okishige MD, FHRS , Kenzo Hirao MD","doi":"10.1016/j.hrthm.2025.03.1989","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>During atypical atrioventricular nodal reentrant tachycardia<span> (AVNRT), the earliest atrial activation site following retrograde slow pathway (SP) conduction is at the atrial exit of the left inferior extension (LIE) in the coronary sinus (CS) or the right inferior extension (RIE) on the tricuspid annulus (TA).</span></div></div><div><h3>Objective</h3><div>The purpose of this study was to assess the validity of a conventional 2-catheter (His bundle and CS) mapping method for localizing the atrial ends of these extensions.</div></div><div><h3>Methods</h3><div>We retrospectively evaluated the efficiency of electrode placement-based mapping of the LIE and RIE in atypical AVNRT using electroanatomic 3-dimensional (3D) mapping validation.</div></div><div><h3>Results</h3><div>Among 19 atypical AVNRTs (15 fast/slow, 4 slow/slow) in 14 patients (9 female; age 59 ± 17 years), 8 AVNRTs had LIE involvement and 11 had RIE. The 8 LIE exits were inside the CS, and localization by 3D mapping and CS electrode catheter matched in all. RIE exits were on the posterior TA where electrode catheters are conventionally not placed, requiring 3D mapping for accurate localization. During retrograde RIE conduction, CS ostium activated earlier than His-bundle electrogram (HBE) in 7 RIEs, HBE was earlier in 1, and they were simultaneous in 3, resulting in the presence of RIE being missed in 4 of 11 AVNRTs (36%) using current diagnostic criteria. The CS ostium and His-bundle activation times were determined by their relative closeness to the RIE exit.</div></div><div><h3>Conclusion</h3><div>Conventionally placed electrode catheter mapping in atypical AVNRT was able to identify 100% of LIEs but only 64% of RIEs. It is critical to place a catheter on the TA.</div></div>","PeriodicalId":12886,"journal":{"name":"Heart rhythm","volume":"22 9","pages":"Pages 2374-2381"},"PeriodicalIF":5.7000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart rhythm","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1547527125022519","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
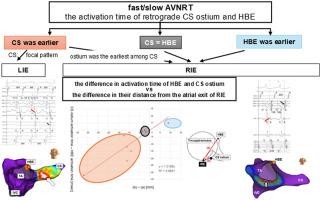
During atypical atrioventricular nodal reentrant tachycardia (AVNRT), the earliest atrial activation site following retrograde slow pathway (SP) conduction is at the atrial exit of the left inferior extension (LIE) in the coronary sinus (CS) or the right inferior extension (RIE) on the tricuspid annulus (TA).
Objective
The purpose of this study was to assess the validity of a conventional 2-catheter (His bundle and CS) mapping method for localizing the atrial ends of these extensions.
Methods
We retrospectively evaluated the efficiency of electrode placement-based mapping of the LIE and RIE in atypical AVNRT using electroanatomic 3-dimensional (3D) mapping validation.
Results
Among 19 atypical AVNRTs (15 fast/slow, 4 slow/slow) in 14 patients (9 female; age 59 ± 17 years), 8 AVNRTs had LIE involvement and 11 had RIE. The 8 LIE exits were inside the CS, and localization by 3D mapping and CS electrode catheter matched in all. RIE exits were on the posterior TA where electrode catheters are conventionally not placed, requiring 3D mapping for accurate localization. During retrograde RIE conduction, CS ostium activated earlier than His-bundle electrogram (HBE) in 7 RIEs, HBE was earlier in 1, and they were simultaneous in 3, resulting in the presence of RIE being missed in 4 of 11 AVNRTs (36%) using current diagnostic criteria. The CS ostium and His-bundle activation times were determined by their relative closeness to the RIE exit.
Conclusion
Conventionally placed electrode catheter mapping in atypical AVNRT was able to identify 100% of LIEs but only 64% of RIEs. It is critical to place a catheter on the TA.
期刊介绍:
HeartRhythm, the official Journal of the Heart Rhythm Society and the Cardiac Electrophysiology Society, is a unique journal for fundamental discovery and clinical applicability.
HeartRhythm integrates the entire cardiac electrophysiology (EP) community from basic and clinical academic researchers, private practitioners, engineers, allied professionals, industry, and trainees, all of whom are vital and interdependent members of our EP community.
The Heart Rhythm Society is the international leader in science, education, and advocacy for cardiac arrhythmia professionals and patients, and the primary information resource on heart rhythm disorders. Its mission is to improve the care of patients by promoting research, education, and optimal health care policies and standards.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
