{"title":"Heterogeneous treatment effects of stress ulcer prophylaxis among ICU patients at risk for gastrointestinal bleeding.","authors":"Yongpeng Xie, Yao Yan, Qixiang Hong, Hui Zheng, Lijuan Cao, Xiaoming Li, Songqiao Liu, Hui Chen","doi":"10.1186/s12916-025-04038-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While randomized clinical trials of stress ulcer prophylaxis (SUP) have generally shown no overall benefit, subgroup analyses suggest the benefit or harm of SUP in specific patients, indicating heterogeneity of treatment effects (HTE). Understanding HTE is crucial for tailoring SUP to individual treatment.</p><p><strong>Methods: </strong>This cohort study included patients admitted to intensive care unit (ICU) with at least one risk factor for clinically important gastrointestinal bleeding (GIB). The primary exposure was the use of SUP within 48 h after ICU entry; the primary outcome was 28-day mortality. We employed conventional subgroup analysis, risk-based analysis, and effect-based analysis to explore the HTE of SUP.</p><p><strong>Results: </strong>A total of 25,475 patients were included, of whom 6199 (24.3%) received SUP, with famotidine being the most commonly prescribed (53.7%). Baseline characteristics were well-balanced between treatment groups after weighting. SUP was not associated with the 28-day mortality in the overall population (median value for the posterior distribution of the odds ratio (OR), 1.03; 95% credible interval (CrI), 0.96-1.11). In conventional subgroups, the impact of SUP on 28-day mortality varied substantially between patients with an age of higher than or equal to 77 years in comparison with other age subgroups (posterior probability of difference in OR, 99.3%), between patients with and without chronic liver disease (posterior probability of difference in OR, 99.9%), between patients with and without coagulopathy (posterior probability of difference in OR, 92.1%), and between patients with and without malignant cancer (posterior probability of difference in OR, 100%). In risk-based analysis, patients at high risk of death exhibited the highest propensity for benefit from SUP (posterior probability of an OR > 1, 1.9%). In effect-based analysis, patients with malignant cancer and a higher Charlson comorbidity index identified at high probability of benefit.</p><p><strong>Conclusions: </strong>Among ICU patients with at least one risk factor for clinically important GIB, those who are younger, have chronic liver disease, coagulopathy, or malignant cancer are more likely to benefit from SUP.</p>","PeriodicalId":9188,"journal":{"name":"BMC Medicine","volume":"23 1","pages":"206"},"PeriodicalIF":8.3000,"publicationDate":"2025-04-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11974205/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12916-025-04038-6","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: While randomized clinical trials of stress ulcer prophylaxis (SUP) have generally shown no overall benefit, subgroup analyses suggest the benefit or harm of SUP in specific patients, indicating heterogeneity of treatment effects (HTE). Understanding HTE is crucial for tailoring SUP to individual treatment.
Methods: This cohort study included patients admitted to intensive care unit (ICU) with at least one risk factor for clinically important gastrointestinal bleeding (GIB). The primary exposure was the use of SUP within 48 h after ICU entry; the primary outcome was 28-day mortality. We employed conventional subgroup analysis, risk-based analysis, and effect-based analysis to explore the HTE of SUP.
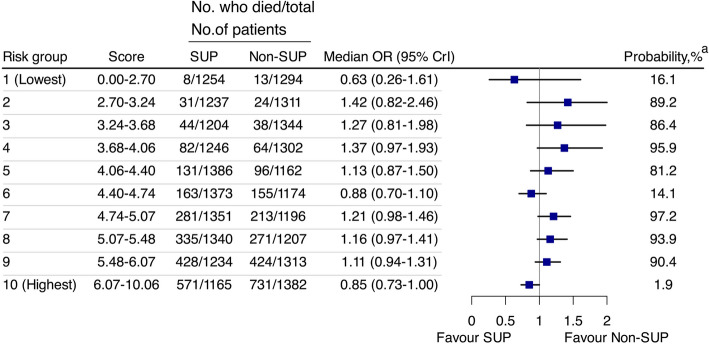
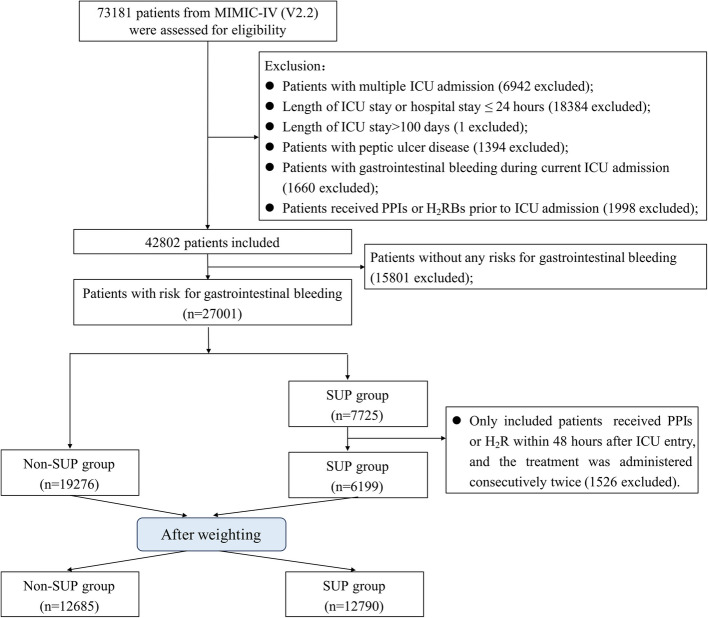
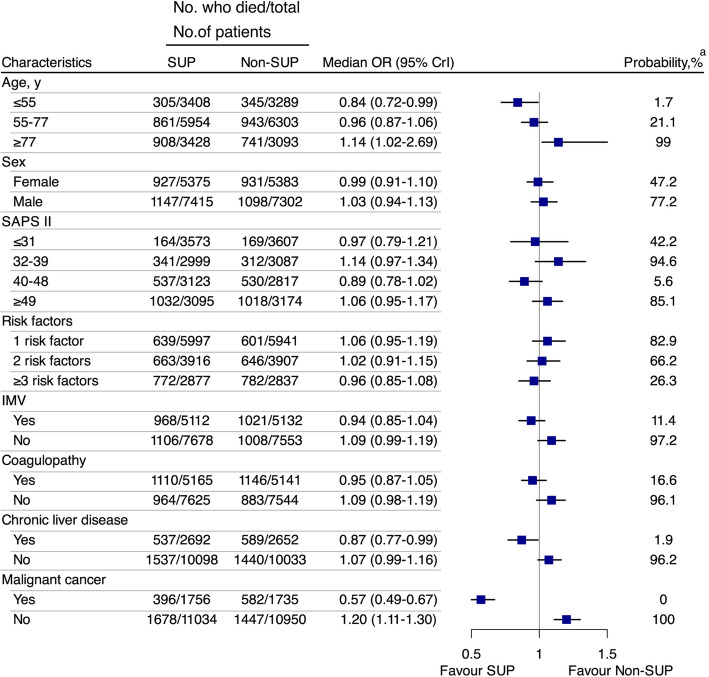
Results: A total of 25,475 patients were included, of whom 6199 (24.3%) received SUP, with famotidine being the most commonly prescribed (53.7%). Baseline characteristics were well-balanced between treatment groups after weighting. SUP was not associated with the 28-day mortality in the overall population (median value for the posterior distribution of the odds ratio (OR), 1.03; 95% credible interval (CrI), 0.96-1.11). In conventional subgroups, the impact of SUP on 28-day mortality varied substantially between patients with an age of higher than or equal to 77 years in comparison with other age subgroups (posterior probability of difference in OR, 99.3%), between patients with and without chronic liver disease (posterior probability of difference in OR, 99.9%), between patients with and without coagulopathy (posterior probability of difference in OR, 92.1%), and between patients with and without malignant cancer (posterior probability of difference in OR, 100%). In risk-based analysis, patients at high risk of death exhibited the highest propensity for benefit from SUP (posterior probability of an OR > 1, 1.9%). In effect-based analysis, patients with malignant cancer and a higher Charlson comorbidity index identified at high probability of benefit.
Conclusions: Among ICU patients with at least one risk factor for clinically important GIB, those who are younger, have chronic liver disease, coagulopathy, or malignant cancer are more likely to benefit from SUP.
期刊介绍:
BMC Medicine is an open access, transparent peer-reviewed general medical journal. It is the flagship journal of the BMC series and publishes outstanding and influential research in various areas including clinical practice, translational medicine, medical and health advances, public health, global health, policy, and general topics of interest to the biomedical and sociomedical professional communities. In addition to research articles, the journal also publishes stimulating debates, reviews, unique forum articles, and concise tutorials. All articles published in BMC Medicine are included in various databases such as Biological Abstracts, BIOSIS, CAS, Citebase, Current contents, DOAJ, Embase, MEDLINE, PubMed, Science Citation Index Expanded, OAIster, SCImago, Scopus, SOCOLAR, and Zetoc.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
