Markus Andersson, Martin Bäckström, Tord Ivarsson, Maria Råstam, Håkan Jarbin
{"title":"Validity of the Brief Child and Family Phone Interview by comparison with Longitudinal Expert All Data diagnoses in outpatients.","authors":"Markus Andersson, Martin Bäckström, Tord Ivarsson, Maria Råstam, Håkan Jarbin","doi":"10.21307/sjcapp-2018-009","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Brief Child and Family Phone Interview (BCFPI) is a standardized intake and follow-up interview used in child and adolescent mental health services (CAMHS). Although it has shown good validity compared with other measures using parent reports, it has not yet been compared with diagnoses derived from a Longitudinal Expert All Data (LEAD) procedure, which includes information from separate diagnostic interviews with parent(s) and child. The aim was to compare the BCFPI evaluation in an outpatient child and adolescent psychiatry setting with an evaluation derived from a LEAD procedure.</p><p><strong>Methods: </strong>At four Swedish outpatient CAMHS, 267 patients were interviewed at intake with the BCFPI. Within six weeks, patients and parents were interviewed separately with the 2009 version of the semi-structured Kiddie Schedule for Affective Disorders and Schizophrenia for School-age Children, Present and Lifetime Version (K-SADS-PL) and parents completed the Child Behavior Checklist (CBCL). LEAD diagnoses were subsequently determined by two senior clinicians based on 1.2 years of clinical records including the K-SADS-PL and ensuing information from further assessments, psychological tests, information from teachers and other informants as well as treatment outcome. The Diagnostic and Statistical Manual of Mental Disorders subscales from the CBCL and the subscales from the BCFPI were compared with LEAD diagnoses. These measured symptoms of attention-deficit hyperactivity disorder, oppositional defiant disorder, conduct disorder, separation anxiety disorder, generalized anxiety disorder, and major depressive disorder.</p><p><strong>Results: </strong>The criterion validity for BCFPI versus LEAD diagnoses was fair for oppositional defiant disorder (area under curve, 0.73), generalized anxiety disorder (0.73) and major depressive disorder (0.78), good for attention-deficit hyperactivity disorder (0.81) and conduct disorder (0.83), and excellent for separation anxiety disorder (0.90). The screening properties of BCFPI and CBCL were similar.</p><p><strong>Conclusion: </strong>The BCFPI is a concise and valid tool, performed along with the larger and more established CBCL, in screening for major psychiatric disorders. It is well suited as an intake interview in CAMHS.</p>","PeriodicalId":42655,"journal":{"name":"Scandinavian Journal of Child and Adolescent Psychiatry and Psychology","volume":"6 2","pages":"83-90"},"PeriodicalIF":1.0000,"publicationDate":"2020-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/65/bc/sjcapp-6-2-083.PMC7703845.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Child and Adolescent Psychiatry and Psychology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21307/sjcapp-2018-009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 5
Abstract
Background: The Brief Child and Family Phone Interview (BCFPI) is a standardized intake and follow-up interview used in child and adolescent mental health services (CAMHS). Although it has shown good validity compared with other measures using parent reports, it has not yet been compared with diagnoses derived from a Longitudinal Expert All Data (LEAD) procedure, which includes information from separate diagnostic interviews with parent(s) and child. The aim was to compare the BCFPI evaluation in an outpatient child and adolescent psychiatry setting with an evaluation derived from a LEAD procedure.
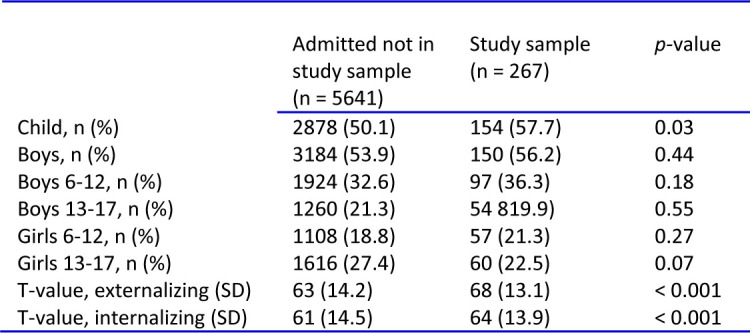
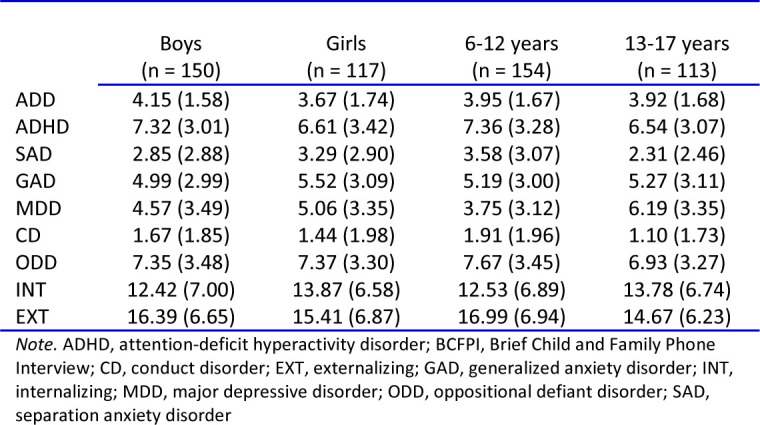
Methods: At four Swedish outpatient CAMHS, 267 patients were interviewed at intake with the BCFPI. Within six weeks, patients and parents were interviewed separately with the 2009 version of the semi-structured Kiddie Schedule for Affective Disorders and Schizophrenia for School-age Children, Present and Lifetime Version (K-SADS-PL) and parents completed the Child Behavior Checklist (CBCL). LEAD diagnoses were subsequently determined by two senior clinicians based on 1.2 years of clinical records including the K-SADS-PL and ensuing information from further assessments, psychological tests, information from teachers and other informants as well as treatment outcome. The Diagnostic and Statistical Manual of Mental Disorders subscales from the CBCL and the subscales from the BCFPI were compared with LEAD diagnoses. These measured symptoms of attention-deficit hyperactivity disorder, oppositional defiant disorder, conduct disorder, separation anxiety disorder, generalized anxiety disorder, and major depressive disorder.
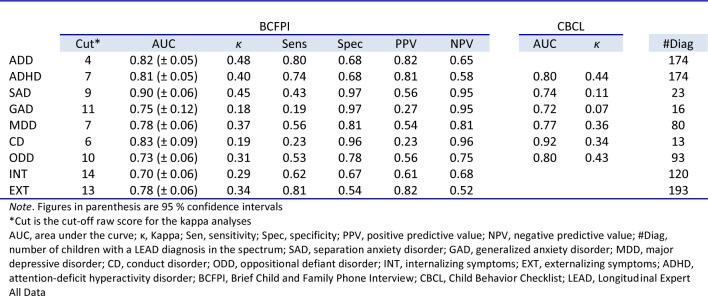
Results: The criterion validity for BCFPI versus LEAD diagnoses was fair for oppositional defiant disorder (area under curve, 0.73), generalized anxiety disorder (0.73) and major depressive disorder (0.78), good for attention-deficit hyperactivity disorder (0.81) and conduct disorder (0.83), and excellent for separation anxiety disorder (0.90). The screening properties of BCFPI and CBCL were similar.
Conclusion: The BCFPI is a concise and valid tool, performed along with the larger and more established CBCL, in screening for major psychiatric disorders. It is well suited as an intake interview in CAMHS.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
