Ryan Guffey, Grace Keane, Austin Y Ha, Rajiv Parikh, Elizabeth Odom, Li Zhang, Terence M Myckatyn
{"title":"Enhanced Recovery With Paravertebral and Transversus Abdominis Plane Blocks in Microvascular Breast Reconstruction.","authors":"Ryan Guffey, Grace Keane, Austin Y Ha, Rajiv Parikh, Elizabeth Odom, Li Zhang, Terence M Myckatyn","doi":"10.1177/1178223420967365","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We have shown previously that a preoperative paravertebral nerve block is associated with improved postoperative recovery in microvascular breast reconstruction. The purpose of this study was to compare the outcomes of a complete enhanced recovery after surgery (ERAS) protocol with complete regional anesthesia coverage to our traditional care with paravertebral block.</p><p><strong>Patients and methods: </strong>This was a retrospective cohort study of 83 patients who underwent autologous breast reconstruction by T.M.M. between May 2014 and February 2018 at a tertiary academic center. Patients in the ERAS group were additionally administered acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), gabapentin, a transversus abdominis plane block (liposomal or plain bupivacaine), and primarily oral opioids postoperatively. The patients were mobilized earlier with more rapid diet progression. All patients received a preoperative paravertebral block.</p><p><strong>Results: </strong>Forty-four patients in the ERAS cohort were compared with 39 retrospective controls. The 2 groups were similar with respect to demographics and comorbidities. The ERAS cohort required significantly less opioids (291 vs 707 mg oral morphine equivalent, <i>P</i> < .0001) with unchanged postoperative pain scores and a shorter time to oral only opioid use (16.0 vs 78.2 hours, <i>P</i> < .0001). Median length of stay (3.20 vs 4.62, <i>P</i> < .0001) and time to independent ambulation (1.86 vs 2.88, <i>P</i> < .0001) were also significantly decreased in the ERAS cohort. Liposomal bupivacaine use did not significantly affect the results (<i>P</i> ⩾ .2).</p><p><strong>Conclusions: </strong>Implementation of a robust enhanced recovery protocol with complete regional anesthesia coverage was associated with significantly decreased opioid use despite unchanged pain scores, with improved markers of recovery including length of stay, time to oral only narcotics, and time to independent ambulation.</p>","PeriodicalId":9163,"journal":{"name":"Breast Cancer : Basic and Clinical Research","volume":"14 ","pages":"1178223420967365"},"PeriodicalIF":1.9000,"publicationDate":"2020-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1178223420967365","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer : Basic and Clinical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1178223420967365","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 4
Abstract
Purpose: We have shown previously that a preoperative paravertebral nerve block is associated with improved postoperative recovery in microvascular breast reconstruction. The purpose of this study was to compare the outcomes of a complete enhanced recovery after surgery (ERAS) protocol with complete regional anesthesia coverage to our traditional care with paravertebral block.
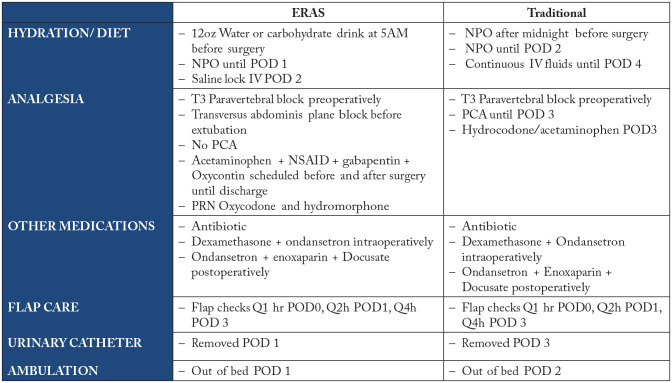
Patients and methods: This was a retrospective cohort study of 83 patients who underwent autologous breast reconstruction by T.M.M. between May 2014 and February 2018 at a tertiary academic center. Patients in the ERAS group were additionally administered acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), gabapentin, a transversus abdominis plane block (liposomal or plain bupivacaine), and primarily oral opioids postoperatively. The patients were mobilized earlier with more rapid diet progression. All patients received a preoperative paravertebral block.
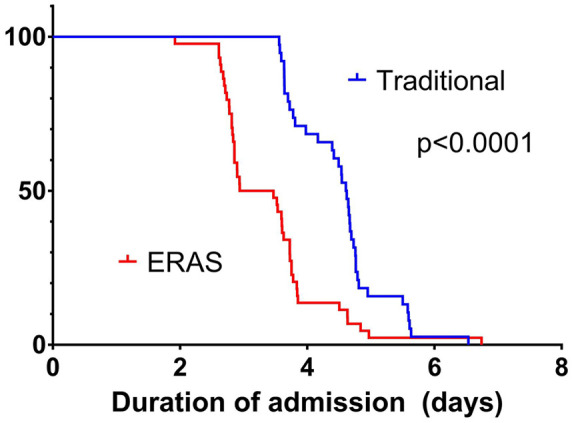
Results: Forty-four patients in the ERAS cohort were compared with 39 retrospective controls. The 2 groups were similar with respect to demographics and comorbidities. The ERAS cohort required significantly less opioids (291 vs 707 mg oral morphine equivalent, P < .0001) with unchanged postoperative pain scores and a shorter time to oral only opioid use (16.0 vs 78.2 hours, P < .0001). Median length of stay (3.20 vs 4.62, P < .0001) and time to independent ambulation (1.86 vs 2.88, P < .0001) were also significantly decreased in the ERAS cohort. Liposomal bupivacaine use did not significantly affect the results (P ⩾ .2).
Conclusions: Implementation of a robust enhanced recovery protocol with complete regional anesthesia coverage was associated with significantly decreased opioid use despite unchanged pain scores, with improved markers of recovery including length of stay, time to oral only narcotics, and time to independent ambulation.
目的:我们之前已经表明,术前椎旁神经阻滞与微血管乳房重建术后恢复的改善有关。本研究的目的是比较具有完全区域麻醉覆盖的手术后完全增强恢复(ERAS)方案与我们传统的椎旁阻滞治疗的结果。患者和方法:这是一项回顾性队列研究,纳入了2014年5月至2018年2月在某三级学术中心接受tmm自体乳房重建术的83例患者。ERAS组患者术后额外给予对乙酰氨基酚、非甾体抗炎药(NSAIDs)、加巴喷丁、经腹平面阻滞(脂质体或普通布比卡因)和主要口服阿片类药物。患者活动更早,饮食进展更快。所有患者术前均接受椎旁阻滞。结果:44例ERAS队列患者与39例回顾性对照进行了比较。两组在人口统计学和合并症方面相似。ERAS队列需要明显更少的阿片类药物(291 vs 707 mg口服吗啡当量,P P P P P小于0.2)。结论:尽管疼痛评分不变,但实施具有完全区域麻醉覆盖的强大增强恢复方案可显著减少阿片类药物的使用,改善恢复指标,包括住院时间、仅口服麻醉剂的时间和独立行走的时间。
期刊介绍:
Breast Cancer: Basic and Clinical Research is an international, open access, peer-reviewed, journal which considers manuscripts on all areas of breast cancer research and treatment. We welcome original research, short notes, case studies and review articles related to breast cancer-related research. Specific areas of interest include, but are not limited to, breast cancer sub types, pathobiology, metastasis, genetics and epigenetics, mammary gland biology, breast cancer models, prevention, detection, therapy and clinical interventions, and epidemiology and population genetics.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
