Jing Miao, Mary E Fidler, Samih H Nasr, Christopher P Larsen, Ziad M Zoghby
{"title":"Membranous nephropathy in a patient with coronavirus disease 2019 (COVID-19): A case report.","authors":"Jing Miao, Mary E Fidler, Samih H Nasr, Christopher P Larsen, Ziad M Zoghby","doi":"10.5414/CNCS110379","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Though respiratory, immune, and coagulation systems are major targets of coronavirus disease 2019 (COVID-19), kidney dysfunction, presenting with acute kidney injury (AKI), is also common. Most AKI cases in COVID-19 manifest as acute tubular injury (ATI) in conjunction with multiorgan failure. While initial renal pathological findings were limited to acute tubular necrosis and collapsing glomerulopathy, a recent case series reported a larger spectrum of findings.</p><p><strong>Case report: </strong>Here, we report a case of membranous nephropathy (MN) in an 81-year-old Hispanic man with underlying chronic kidney disease (CKD) stage 3 who developed ATI in the setting of COVID-19. The patient was hospitalized for hypoxic respiratory failure in the setting of AKI stage 3 with serum creatinine 7.1 mg/dL 6 days after a positive-SARS-CoV-2 screening. He was found to have nephrotic range proteinuria, glycosuria (with normal serum glucose), anemia, and hypoalbuminemia. Kidney biopsy showed ATI and early MN. Workup for primary and secondary MN was unrevealing, and serum PLA2R antibody was negative. No viral particles were observed in podocytes.</p><p><strong>Conclusion: </strong>Although the MN could be incidental, this observation raises the question of whether SARS-CoV-2 infection can trigger or worsen an underlying MN from an exaggerated immune response associated with COVID-19.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"9 ","pages":"11-18"},"PeriodicalIF":0.0000,"publicationDate":"2021-02-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7901357/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110379","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Though respiratory, immune, and coagulation systems are major targets of coronavirus disease 2019 (COVID-19), kidney dysfunction, presenting with acute kidney injury (AKI), is also common. Most AKI cases in COVID-19 manifest as acute tubular injury (ATI) in conjunction with multiorgan failure. While initial renal pathological findings were limited to acute tubular necrosis and collapsing glomerulopathy, a recent case series reported a larger spectrum of findings.
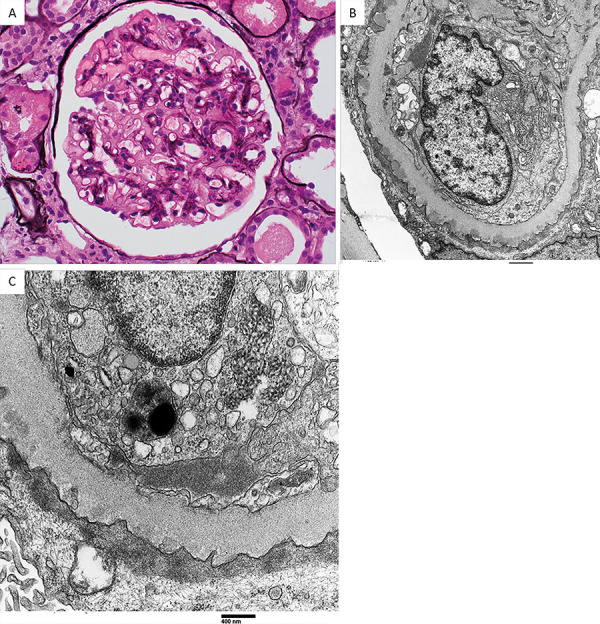
Case report: Here, we report a case of membranous nephropathy (MN) in an 81-year-old Hispanic man with underlying chronic kidney disease (CKD) stage 3 who developed ATI in the setting of COVID-19. The patient was hospitalized for hypoxic respiratory failure in the setting of AKI stage 3 with serum creatinine 7.1 mg/dL 6 days after a positive-SARS-CoV-2 screening. He was found to have nephrotic range proteinuria, glycosuria (with normal serum glucose), anemia, and hypoalbuminemia. Kidney biopsy showed ATI and early MN. Workup for primary and secondary MN was unrevealing, and serum PLA2R antibody was negative. No viral particles were observed in podocytes.
Conclusion: Although the MN could be incidental, this observation raises the question of whether SARS-CoV-2 infection can trigger or worsen an underlying MN from an exaggerated immune response associated with COVID-19.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
