Experience of treating pediatric hepatoblastoma at King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia – Timely surgical intervention playing a key role
Ibrahim AlFawaz , Basheer Ahmed , Afshan Ali , Mouhab Ayas , Amani AlKofide , Zakaria Habib , Khawar Siddiqui
{"title":"Experience of treating pediatric hepatoblastoma at King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia – Timely surgical intervention playing a key role","authors":"Ibrahim AlFawaz , Basheer Ahmed , Afshan Ali , Mouhab Ayas , Amani AlKofide , Zakaria Habib , Khawar Siddiqui","doi":"10.1016/j.ijpam.2020.11.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Many studies have demonstrated that outcome in patients with hepatoblastoma is determined by tumor resectability and the presence or absence of metastatic disease.</p></div><div><h3>Purpose</h3><p>To evaluate and disseminate information on diagnosis, treatment, and outcome of hepatoblastoma patients at a tertiary care hospital in Saudi Arabia.</p></div><div><h3>Patients and methods</h3><p>Twenty-four pediatric patients with hepatoblastoma were treated at our institution between January 2005 and December 2012. The majority of our patients were stage III and above, while one-third of them presented with metastatic disease. Four (16.7%) had vascular invasion. Two-thirds of our patients (n = 16, 66.7%) had alpha-fetoprotein (AFP) level above 100,000 ng/mL. Twenty-one patients underwent surgery; two had upfront surgery before getting any chemotherapy, and 15 had surgery on schedule after pre-operative chemotherapy. Four patients had delayed surgery as the tumor was not resectable and received extra cycles of chemotherapy. Chemotherapy regimens used were based on SIOPEL study protocols until 2011 and Children’s Oncology Group (COG) protocol from 2012 onwards. Relapse, progressive disease, or death from any cause were defined as events.</p></div><div><h3>Results</h3><p>Five-year overall survival (OS) of the cohort over a median follow-up time of 56.1 months was 70.6% ± 9.4% with seven (29.2%) events of mortality. No significant difference was found for age at diagnosis (less than 2 years vs. more), stage of disease, AFP levels (less than 100,000 vs. more), vascular invasion, or presence of metastatic disease at presentation in terms of OS. However, children receiving upfront or scheduled as-per-protocol surgery fared better than those who had delayed surgery (as the tumor was not resectable and they received extra cycles of chemotherapy) or did not undergo any surgery (<em>P-Value</em> .001).</p></div><div><h3>Conclusion</h3><p>Favorable survival outcome could be achieved with complete tumor excision and adjuvant chemotherapy. Inability to perform surgical excision was the single most important predictor of mortality in our patients.</p></div>","PeriodicalId":36646,"journal":{"name":"International Journal of Pediatrics and Adolescent Medicine","volume":"8 1","pages":"Pages 39-43"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijpam.2020.11.001","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Pediatrics and Adolescent Medicine","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2352646720300879","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/11/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background
Many studies have demonstrated that outcome in patients with hepatoblastoma is determined by tumor resectability and the presence or absence of metastatic disease.
Purpose
To evaluate and disseminate information on diagnosis, treatment, and outcome of hepatoblastoma patients at a tertiary care hospital in Saudi Arabia.
Patients and methods
Twenty-four pediatric patients with hepatoblastoma were treated at our institution between January 2005 and December 2012. The majority of our patients were stage III and above, while one-third of them presented with metastatic disease. Four (16.7%) had vascular invasion. Two-thirds of our patients (n = 16, 66.7%) had alpha-fetoprotein (AFP) level above 100,000 ng/mL. Twenty-one patients underwent surgery; two had upfront surgery before getting any chemotherapy, and 15 had surgery on schedule after pre-operative chemotherapy. Four patients had delayed surgery as the tumor was not resectable and received extra cycles of chemotherapy. Chemotherapy regimens used were based on SIOPEL study protocols until 2011 and Children’s Oncology Group (COG) protocol from 2012 onwards. Relapse, progressive disease, or death from any cause were defined as events.
Results
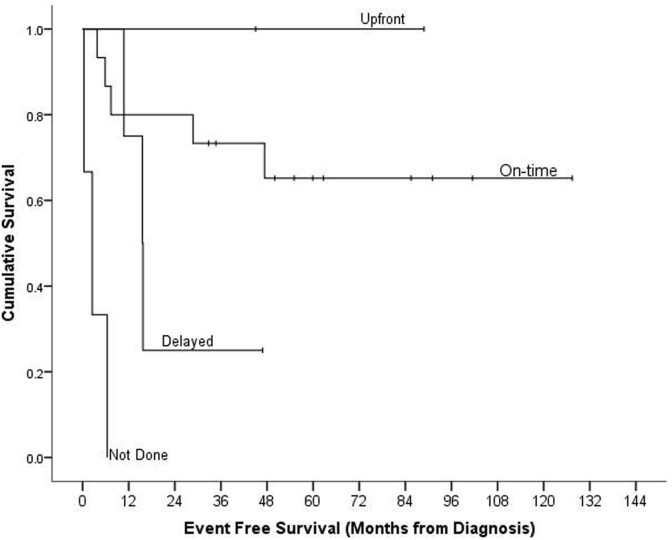
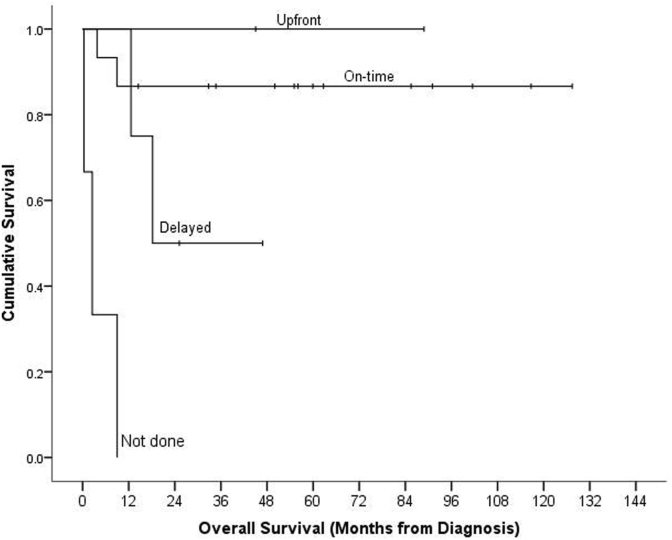
Five-year overall survival (OS) of the cohort over a median follow-up time of 56.1 months was 70.6% ± 9.4% with seven (29.2%) events of mortality. No significant difference was found for age at diagnosis (less than 2 years vs. more), stage of disease, AFP levels (less than 100,000 vs. more), vascular invasion, or presence of metastatic disease at presentation in terms of OS. However, children receiving upfront or scheduled as-per-protocol surgery fared better than those who had delayed surgery (as the tumor was not resectable and they received extra cycles of chemotherapy) or did not undergo any surgery (P-Value .001).
Conclusion
Favorable survival outcome could be achieved with complete tumor excision and adjuvant chemotherapy. Inability to perform surgical excision was the single most important predictor of mortality in our patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
