A randomized prospective study comparing acute toxicity, compliance and objective response rate between simultaneous integrated boost and sequential intensity-modulated radiotherapy for locally advanced head and neck cancer.
{"title":"A randomized prospective study comparing acute toxicity, compliance and objective response rate between simultaneous integrated boost and sequential intensity-modulated radiotherapy for locally advanced head and neck cancer.","authors":"Akanksha Grover, Tej Prakash Soni, Nidhi Patni, Dinesh Kumar Singh, Naresh Jakhotia, Anil Kumar Gupta, Lalit Mohan Sharma, Shantanu Sharma, Ravindra Singh Gothwal","doi":"10.3857/roj.2020.01018","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Intensity-modulated radiotherapy (IMRT) provides higher dose to target volumes and limits the dose to normal tissues. IMRT may be applied using either simultaneous integrated boost (SIB-IMRT) or sequential boost (SEQ-IMRT) technique. The objectives of this study were to compare acute toxicity and objective response rates between SIB-IMRT and SEQ-IMRT in patients with locally advanced head and neck cancer.</p><p><strong>Materials and methods: </strong>Total 110 patients with locally advanced carcinoma of oropharynx, hypopharynx, and larynx were randomized equally into the two arms (SIB-IMRT vs. SEQ-IMRT). Patients in SIB-IMRT arm received dose of 66 Gy in 30 fractions, 5 days a week, over 6 weeks. SEQ-IMRT arm's patients received 70 Gy in 35 fractions over 7 weeks. Weekly concurrent cisplatin chemotherapy was given in both arms. Patients were assessed for acute toxicities during the treatment and for objective response at 3 months after the radiotherapy.</p><p><strong>Results: </strong>Grade 3 dysphagia was significantly more with SIB-IMRT compared to SEQ-IMRT (72% vs. 41.2%; p = 0.006) but other toxicities including mucositis, dermatitis, xerostomia, weight-loss, incidence of nasogastric tube intubation and hospitalization for supportive management were similar in both the arms. Patients in SIB-IMRT arm showed better treatment-compliance and had significantly less treatment-interruption compared to SEQ-IMRT arm (p = 0.028). Objective response rates were similar in both the arms (p = 0.783).</p><p><strong>Conclusion: </strong>Concurrent chemoradiation with SIB-IMRT for locally advanced head and neck cancer is well-tolerated and results in better treatment-compliance, similar objective response rates, comparable incidence of mucositis and higher incidence of grade 3 dysphagia compared to SEQ-IMRT.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"39 1","pages":"15-23"},"PeriodicalIF":2.2000,"publicationDate":"2021-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/cf/roj-2020-01018.PMC8024186.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2020.01018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/3/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Intensity-modulated radiotherapy (IMRT) provides higher dose to target volumes and limits the dose to normal tissues. IMRT may be applied using either simultaneous integrated boost (SIB-IMRT) or sequential boost (SEQ-IMRT) technique. The objectives of this study were to compare acute toxicity and objective response rates between SIB-IMRT and SEQ-IMRT in patients with locally advanced head and neck cancer.
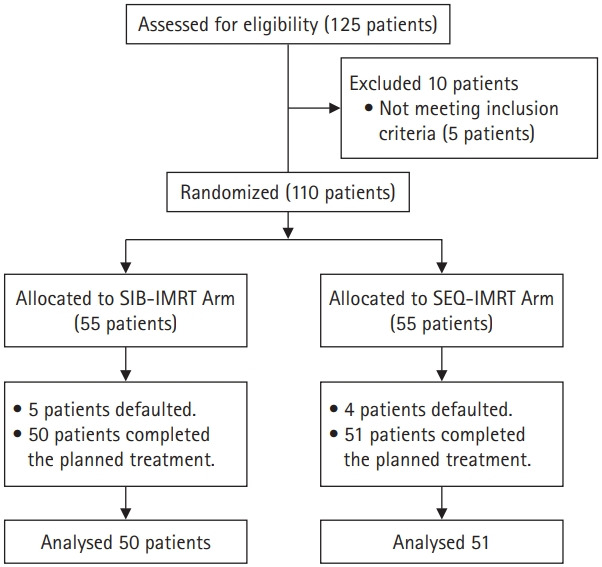
Materials and methods: Total 110 patients with locally advanced carcinoma of oropharynx, hypopharynx, and larynx were randomized equally into the two arms (SIB-IMRT vs. SEQ-IMRT). Patients in SIB-IMRT arm received dose of 66 Gy in 30 fractions, 5 days a week, over 6 weeks. SEQ-IMRT arm's patients received 70 Gy in 35 fractions over 7 weeks. Weekly concurrent cisplatin chemotherapy was given in both arms. Patients were assessed for acute toxicities during the treatment and for objective response at 3 months after the radiotherapy.
Results: Grade 3 dysphagia was significantly more with SIB-IMRT compared to SEQ-IMRT (72% vs. 41.2%; p = 0.006) but other toxicities including mucositis, dermatitis, xerostomia, weight-loss, incidence of nasogastric tube intubation and hospitalization for supportive management were similar in both the arms. Patients in SIB-IMRT arm showed better treatment-compliance and had significantly less treatment-interruption compared to SEQ-IMRT arm (p = 0.028). Objective response rates were similar in both the arms (p = 0.783).
Conclusion: Concurrent chemoradiation with SIB-IMRT for locally advanced head and neck cancer is well-tolerated and results in better treatment-compliance, similar objective response rates, comparable incidence of mucositis and higher incidence of grade 3 dysphagia compared to SEQ-IMRT.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
