Diagnosing idiopathic learning disability: a cost-effectiveness analysis of microarray technology in the National Health Service of the United Kingdom.
Sarah Wordsworth, James Buchanan, Regina Regan, Val Davison, Kim Smith, Sara Dyer, Carolyn Campbell, Edward Blair, Eddy Maher, Jenny Taylor, Samantha J L Knight
{"title":"Diagnosing idiopathic learning disability: a cost-effectiveness analysis of microarray technology in the National Health Service of the United Kingdom.","authors":"Sarah Wordsworth, James Buchanan, Regina Regan, Val Davison, Kim Smith, Sara Dyer, Carolyn Campbell, Edward Blair, Eddy Maher, Jenny Taylor, Samantha J L Knight","doi":"10.1007/s11568-007-9005-6","DOIUrl":null,"url":null,"abstract":"<p><p>Array based comparative genomic hybridisation (aCGH) is a powerful technique for detecting clinically relevant genome imbalance and can offer 40 to > 1000 times the resolution of karyotyping. Indeed, idiopathic learning disability (ILD) studies suggest that a genome-wide aCGH approach makes 10-15% more diagnoses involving genome imbalance than karyotyping. Despite this, aCGH has yet to be implemented as a routine NHS service. One significant obstacle is the perception that the technology is prohibitively expensive for most standard NHS clinical cytogenetics laboratories. To address this, we investigated the cost-effectiveness of aCGH versus standard cytogenetic analysis for diagnosing idiopathic learning disability (ILD) in the NHS. Cost data from four participating genetics centres were collected and analysed. In a single test comparison, the average cost of aCGH was pound442 and the average cost of karyotyping was pound117 with array costs contributing most to the cost difference. This difference was not a key barrier when the context of follow up diagnostic tests was considered. Indeed, in a hypothetical cohort of 100 ILD children, aCGH was found to cost less per diagnosis ( pound3,118) than a karyotyping and multi-telomere FISH approach ( pound4,957). We conclude that testing for genomic imbalances in ILD using microarray technology is likely to be cost-effective because long-term savings can be made regardless of a positive (diagnosis) or negative result. Earlier diagnoses save costs of additional diagnostic tests. Negative results are cost-effective in minimising follow-up test choice. The use of aCGH in routine clinical practice warrants serious consideration by healthcare providers.</p>","PeriodicalId":87975,"journal":{"name":"Genomic medicine","volume":"1 1-2","pages":"35-45"},"PeriodicalIF":3.5000,"publicationDate":"2007-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s11568-007-9005-6","citationCount":"37","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Genomic medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s11568-007-9005-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2007/6/5 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"EDUCATION & EDUCATIONAL RESEARCH","Score":null,"Total":0}
引用次数: 37
Abstract
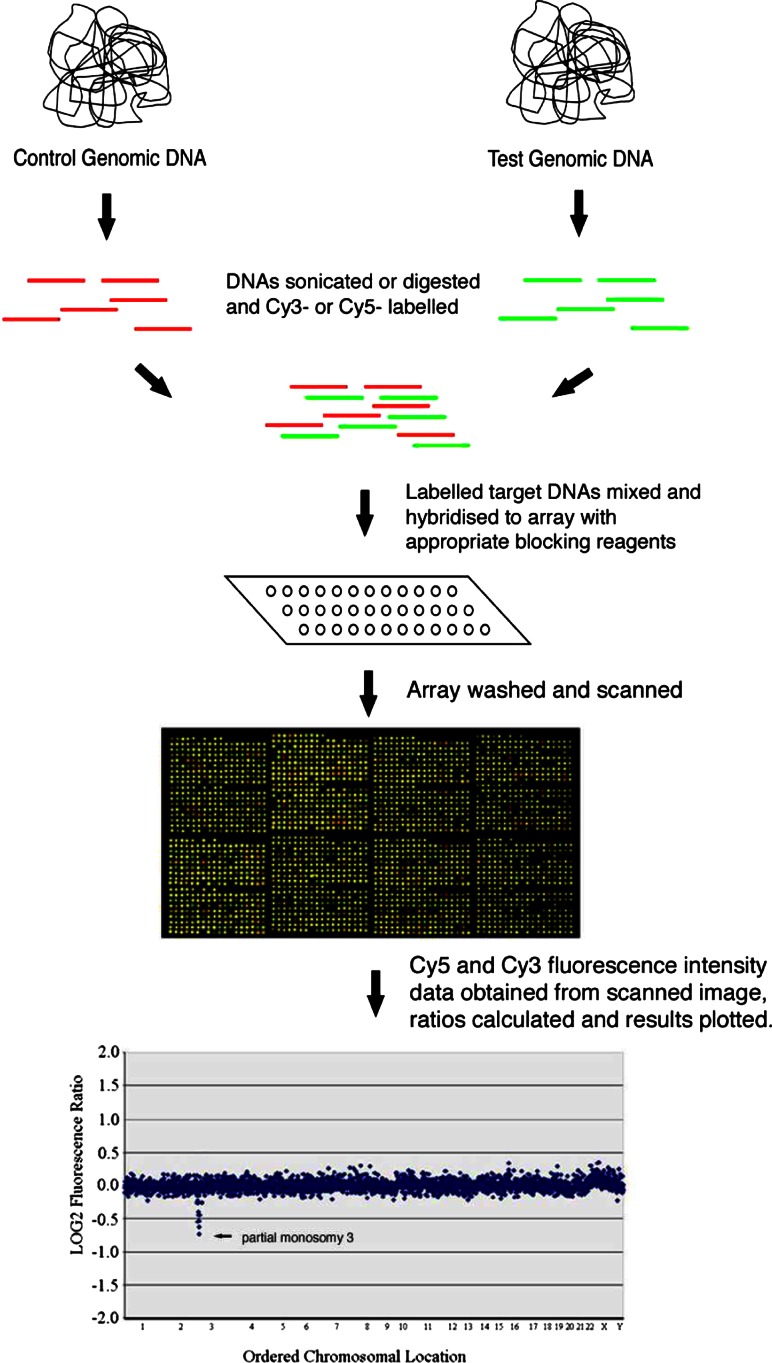
Array based comparative genomic hybridisation (aCGH) is a powerful technique for detecting clinically relevant genome imbalance and can offer 40 to > 1000 times the resolution of karyotyping. Indeed, idiopathic learning disability (ILD) studies suggest that a genome-wide aCGH approach makes 10-15% more diagnoses involving genome imbalance than karyotyping. Despite this, aCGH has yet to be implemented as a routine NHS service. One significant obstacle is the perception that the technology is prohibitively expensive for most standard NHS clinical cytogenetics laboratories. To address this, we investigated the cost-effectiveness of aCGH versus standard cytogenetic analysis for diagnosing idiopathic learning disability (ILD) in the NHS. Cost data from four participating genetics centres were collected and analysed. In a single test comparison, the average cost of aCGH was pound442 and the average cost of karyotyping was pound117 with array costs contributing most to the cost difference. This difference was not a key barrier when the context of follow up diagnostic tests was considered. Indeed, in a hypothetical cohort of 100 ILD children, aCGH was found to cost less per diagnosis ( pound3,118) than a karyotyping and multi-telomere FISH approach ( pound4,957). We conclude that testing for genomic imbalances in ILD using microarray technology is likely to be cost-effective because long-term savings can be made regardless of a positive (diagnosis) or negative result. Earlier diagnoses save costs of additional diagnostic tests. Negative results are cost-effective in minimising follow-up test choice. The use of aCGH in routine clinical practice warrants serious consideration by healthcare providers.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
