{"title":"The etiology and prevention of feeding intolerance paralytic ileus--revisiting an old concept.","authors":"Gerald Moss","doi":"10.1186/1750-1164-3-3","DOIUrl":null,"url":null,"abstract":"<p><p>Gastro-intestinal (G-I) motility is impaired (\"paralytic ileus\") after abdominal surgery. Premature feeding attempts delay recovery by inducing \"feeding intolerance,\" especially abdominal distention that compromises respiration. Controlled studies (e.g., from Sloan-Kettering Memorial Hospital) have lead to recommendations that patients not be fed soon after major abdominal surgery to avoid this complication. We postulate that when total fluid inflow of feedings, digestive secretions, and swallowed air outstrip peristaltic outflow from the feeding site, fluid accumulates. This localized stagnation triggers G-I vagal reflexes that further slow the already sluggish gut, leading to generalized abdominal distention. Similarly, vagal cardiovascular reflexes in susceptible subjects could account for the 1:1,000 incidence of unexplained bowel necrosis reported with enteral feeding. We re-evaluated our data, which supports this postulated mechanism for the induction of \"feeding intolerance.\" We had focused our efforts on postoperative enteral nutrition, with the largest reported series of immediate feeding of at least 100 kcal/hour after major surgery. We found that this complication can be avoided consistently by monitoring inflow versus peristaltic outflow, immediately removing any potential excess from the feeding site. We fed intraduodenally immediately following \"open\" surgery for 31 colectomy and 160 consecutive cholecystectomy patients. The duodenum was aspirated simultaneously just proximal to the feeding site, efficiently removing all swallowed air and excess feedings. To salvage digestive secretions, the degassed aspirate was re-introduced manually (and later automatically) via a separate feeding channel. Hourly assays were performed for nitrogen balance, serum amino acids, and for the presence of removed feedings in the aspirate. The colectomy patients had X-ray motility studies initiated 5-17 hours after surgery. Clinically normal motility and absorption resumed within two hours. Fed BaSO4 traversed secure anastomoses, to exit in bowel movements within 24-48 hours of colectomy. All patients were in positive protein balance within 2-24 hours, with elevated serum amino acids levels and without adverse G-I effects. Limiting inflow to match peristaltic outflow from the feeding site consistently prevented \"feeding intolerance.\" These patients received immediate full enteral nutrition, with the most rapid resolution of postoperative paralytic ileus, to date.</p>","PeriodicalId":87428,"journal":{"name":"Annals of surgical innovation and research","volume":"3 ","pages":"3"},"PeriodicalIF":0.0000,"publicationDate":"2009-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2678143/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgical innovation and research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1750-1164-3-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
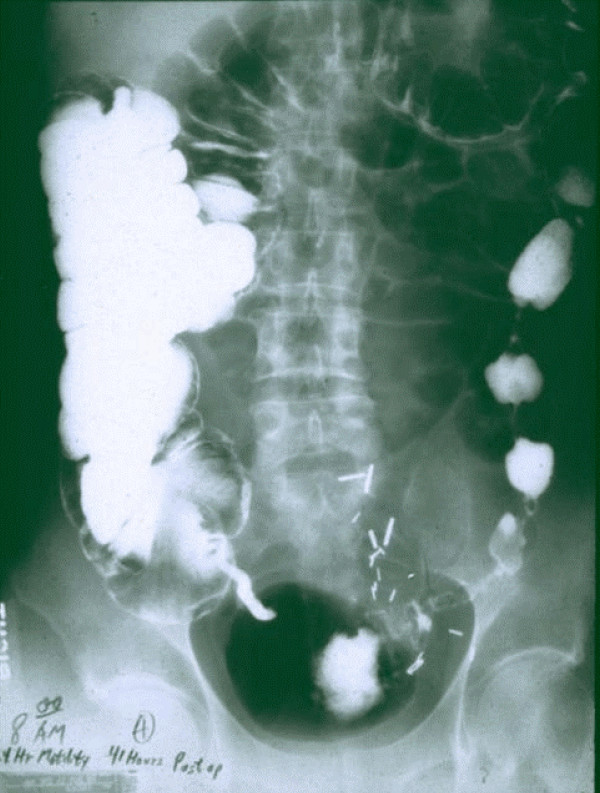
Gastro-intestinal (G-I) motility is impaired ("paralytic ileus") after abdominal surgery. Premature feeding attempts delay recovery by inducing "feeding intolerance," especially abdominal distention that compromises respiration. Controlled studies (e.g., from Sloan-Kettering Memorial Hospital) have lead to recommendations that patients not be fed soon after major abdominal surgery to avoid this complication. We postulate that when total fluid inflow of feedings, digestive secretions, and swallowed air outstrip peristaltic outflow from the feeding site, fluid accumulates. This localized stagnation triggers G-I vagal reflexes that further slow the already sluggish gut, leading to generalized abdominal distention. Similarly, vagal cardiovascular reflexes in susceptible subjects could account for the 1:1,000 incidence of unexplained bowel necrosis reported with enteral feeding. We re-evaluated our data, which supports this postulated mechanism for the induction of "feeding intolerance." We had focused our efforts on postoperative enteral nutrition, with the largest reported series of immediate feeding of at least 100 kcal/hour after major surgery. We found that this complication can be avoided consistently by monitoring inflow versus peristaltic outflow, immediately removing any potential excess from the feeding site. We fed intraduodenally immediately following "open" surgery for 31 colectomy and 160 consecutive cholecystectomy patients. The duodenum was aspirated simultaneously just proximal to the feeding site, efficiently removing all swallowed air and excess feedings. To salvage digestive secretions, the degassed aspirate was re-introduced manually (and later automatically) via a separate feeding channel. Hourly assays were performed for nitrogen balance, serum amino acids, and for the presence of removed feedings in the aspirate. The colectomy patients had X-ray motility studies initiated 5-17 hours after surgery. Clinically normal motility and absorption resumed within two hours. Fed BaSO4 traversed secure anastomoses, to exit in bowel movements within 24-48 hours of colectomy. All patients were in positive protein balance within 2-24 hours, with elevated serum amino acids levels and without adverse G-I effects. Limiting inflow to match peristaltic outflow from the feeding site consistently prevented "feeding intolerance." These patients received immediate full enteral nutrition, with the most rapid resolution of postoperative paralytic ileus, to date.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
