Christophe Schmitt PharmD, Myriam Riek MSc, Katie Winters PharmD, Malte Schutz MD, Susan Grange PharmD, PhD
{"title":"Unexpected Hepatotoxicity of Rifampin and Saquinavir/Ritonavir in Healthy Male Volunteers","authors":"Christophe Schmitt PharmD, Myriam Riek MSc, Katie Winters PharmD, Malte Schutz MD, Susan Grange PharmD, PhD","doi":"10.1111/j.1753-5174.2009.00017.x","DOIUrl":null,"url":null,"abstract":"<p><b>Objectives. </b> Rifampin is a potent inducer of the cytochrome P450 3A4 isoenzyme (CYP3A4) that metabolizes most protease inhibitor (PI) antiretrovirals. This study was designed to evaluate the steady-state pharmacokinetics and tolerability of the coadministration of the PIs saquinavir and ritonavir (a CYP3A4 inhibitor used as a pharmacoenhancer of other PIs) and rifampin when coadministered in healthy HIV-negative volunteers.</p><p><b>Methods. </b> In an open-label, randomized, one sequence, two-period crossover study involving 28 healthy HIV-negative volunteers, arm 1 was randomized to receive saquinavir/ritonavir 1000/100 mg twice daily while arm 2 received rifampin 600 mg once daily for 14 days. Both arms were then to receive concomitant saquinavir/ritonavir and rifampin for 2 additional weeks. Vital signs, electrocardiography, laboratory analyses, and blood levels of total saquinavir, ritonavir, rifampin, and desacetyl-rifampin, the primary metabolite of rifampin, were measured.</p><p><b>Results. </b> In arm 1, 10/14 (71%) and, in arm 2, 11/14 (79%) participants completed the first study phase; eight participants in arm 1 and nine in arm 2 went on to receive both saquinavir/ritonavir and rifampin. Following substantial elevations (≥ grade 2) in hepatic transaminases in participants receiving the coadministered agents, the study was discontinued prematurely. Two participants in arm 1 displayed moderate elevations after five and four doses of rifampin, respectively. In arm 2, all participants experienced severe elevations within 4 days of initiating saquinavir/ritonavir. Clinical symptoms (e.g., nausea, vomiting, abdominal pain, and headache) were more common and severe in arm 2. Clinical symptoms abated and transaminases normalized following drug discontinuation. Limited pharmacokinetic data suggest a possible relationship between transaminase elevation and elevated rifampin and desacetyl-rifampin concentrations.</p><p><b>Conclusions. </b> Although not confirmed in HIV-infected patients, the data indicate that rifampin should not be coadministered with saquinavir/ritonavir.</p>","PeriodicalId":8181,"journal":{"name":"Archives of Drug Information","volume":"2 1","pages":"8-16"},"PeriodicalIF":0.0000,"publicationDate":"2009-03-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1111/j.1753-5174.2009.00017.x","citationCount":"80","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Drug Information","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/j.1753-5174.2009.00017.x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 80
Abstract
Objectives. Rifampin is a potent inducer of the cytochrome P450 3A4 isoenzyme (CYP3A4) that metabolizes most protease inhibitor (PI) antiretrovirals. This study was designed to evaluate the steady-state pharmacokinetics and tolerability of the coadministration of the PIs saquinavir and ritonavir (a CYP3A4 inhibitor used as a pharmacoenhancer of other PIs) and rifampin when coadministered in healthy HIV-negative volunteers.
Methods. In an open-label, randomized, one sequence, two-period crossover study involving 28 healthy HIV-negative volunteers, arm 1 was randomized to receive saquinavir/ritonavir 1000/100 mg twice daily while arm 2 received rifampin 600 mg once daily for 14 days. Both arms were then to receive concomitant saquinavir/ritonavir and rifampin for 2 additional weeks. Vital signs, electrocardiography, laboratory analyses, and blood levels of total saquinavir, ritonavir, rifampin, and desacetyl-rifampin, the primary metabolite of rifampin, were measured.
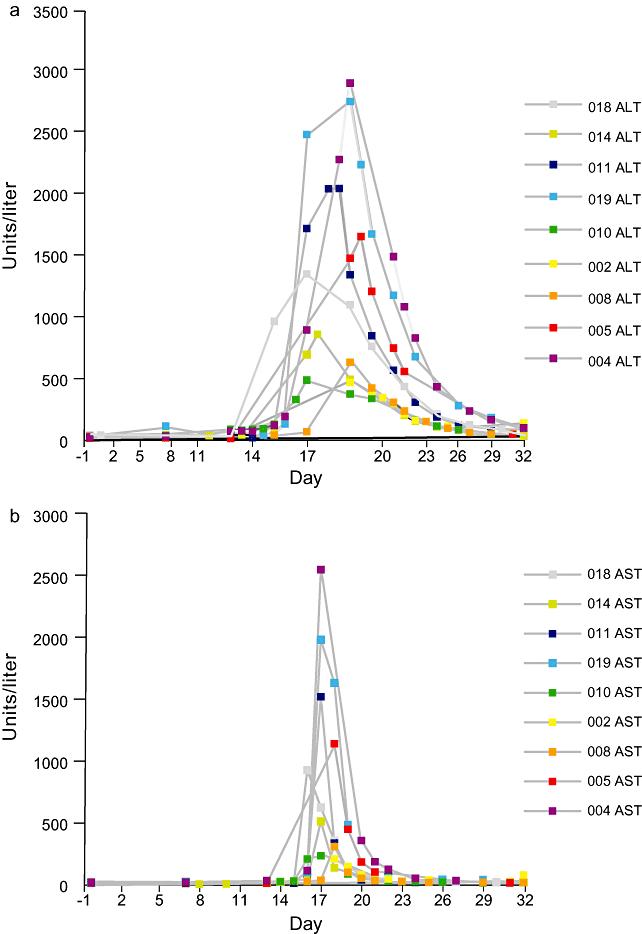
Results. In arm 1, 10/14 (71%) and, in arm 2, 11/14 (79%) participants completed the first study phase; eight participants in arm 1 and nine in arm 2 went on to receive both saquinavir/ritonavir and rifampin. Following substantial elevations (≥ grade 2) in hepatic transaminases in participants receiving the coadministered agents, the study was discontinued prematurely. Two participants in arm 1 displayed moderate elevations after five and four doses of rifampin, respectively. In arm 2, all participants experienced severe elevations within 4 days of initiating saquinavir/ritonavir. Clinical symptoms (e.g., nausea, vomiting, abdominal pain, and headache) were more common and severe in arm 2. Clinical symptoms abated and transaminases normalized following drug discontinuation. Limited pharmacokinetic data suggest a possible relationship between transaminase elevation and elevated rifampin and desacetyl-rifampin concentrations.
Conclusions. Although not confirmed in HIV-infected patients, the data indicate that rifampin should not be coadministered with saquinavir/ritonavir.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
