Sun Young Cho, Anbok Lee, Hee Joo Lee, Jin-Tae Suh
{"title":"Overlapping presence of macroamylasemia and hyperamylasemia in acute pancreatitis.","authors":"Sun Young Cho, Anbok Lee, Hee Joo Lee, Jin-Tae Suh","doi":"10.3343/kjlm.2011.31.2.98","DOIUrl":null,"url":null,"abstract":"Accurate interpretation of elevated amylase levels is essential, especially for patients presenting with an overlapping pancreatic or liver disease or for patients with a history of these diseases [1]. In this study, we have described an unusual case of macroamylasemia that occurred immediately after acute pancreatitis. On March 9, 2010, a 56-yr-old Korean man was admitted to the emergency department because of confusion and delirium. He had previously been hospitalized for 4 months because of alcoholic cirrhosis and had been discharged 5 days prior to this admission. During the 4-month hospitalization, he had received treatment for esophageal variceal bleeding and acute pancreatitis. At that time, his serum amylase levels and lipase levels were 1,171 U/L and 298 U/L, respectively. Abdominal computed tomography images showed mild swelling of the pancreas and a cystic lesion (1.5 cm) in the pancreatic head (Fig. 1). The patient received therapy for acute pancreatitis. Although he showed improvement in symptoms and radiological findings at the time of discharge, on March 4, 2010, the serum amylase levels had increased to 1,882 U/L (Fig. 2). Five days later, the patient was readmitted because of altered mental status. Physical examinations revealed no abdominal pain and no rebound tenderness. The results of the blood biochemistry tests were as follows: total protein, 9.2 g/dL; albumin, 2.9 g/dL; amylase, 2,232 IU/L (25-125 IU/L); lipase, 61 IU/L (5.5-58 IU/L); total bilirubin, 2.39 mg/dL; direct bilirubin, 1.63 mg/dL; AST, 48 IU/L; ALT, 30 IU/L; alkaline phosphatase (ALP), 64 IU/L; gamma-glutamyl transpeptidase (GGT), 29 IU/L; and ammonia, 141 mg/dL. The serological tests yielded the following results: IgG, 3,850 mg/dL (700-1,600 mg/dL) and IgA, 664 mg/dL (70-400 mg/dL). After readmission, the urine amylase level was 54 IU/L (1-352 IU/L), and the amylase-creatinine clearance ratio (ACCR) was calculated to be 0.07%. Macroamylasemia was diagnosed on the basis of these findings. Serum amylase isoenzyme electrophoresis showed that the proportions of P-type and S-type amylases were 75.3% and 24.7%, respectively. Capillary serum protein electrophoresis revealed polyclonal gammopathy with a beta-gamma bridge pattern, which is a typical pattern in liver cirrhosis (Fig. 3). The patient's mental status returned to normal, and he is still in the hospital for continued management of liver cirrhosis. \n \n \n \nFig. 1 \n \nFindings of abdominal computed tomography performed when the patient showed acute pancreatitis. A cystic lesion (arrows, 1.5 cm) in the pancreatic head region (A) and mild swelling of the pancreas (B) are observed. \n \n \n \n \n \nFig. 2 \n \nTrends in the serum amylase and lipase levels from the time of diagnosis of acute pancreatitis (*) to the time of diagnosis of macroamylasemia (**). Serum amylase levels are high for about 4 months, while lipase levels fall near the upper reference limit. ... \n \n \n \n \n \nFig. 3 \n \nSerum amylase isoenzyme electrophoresis (A) and capillary electrophoresis (B and C). (A) The P-type amylase level increased to 1,664.13 IU/L (75.30% of the total amylase concentration). The S-type amylase level is within the reference interval (545.87 ... \n \n \n \nMacroamylasemia has been reported in 2.5% of the patients with hyperamylasemia and in 1% of the general population; approximately 0.4% of the cases in the general population occur in the West [2, 3]. Increased amylase and/or lipase activities were seen in 8% of the patients without pancreatic diseases [4]. In the previous reports, macroamylasemia was mainly reported in patients with disturbed humoral immunity, such as those with celiac disease, multiple myeloma, HIV infection, ulcerative colitis, and rheumatoid arthritis [2, 3, 5-8]. One of the predisposing conditions for macroamylasemia is a polyclonal increase in immunoglobulins (Ig). Some studies have reported that macroamylasemia may decrease or resolve when these underlying diseases are treated, and that the risk for autoimmune or lymphoproliferative diseases is higher in macroamylasemia with light-chain restriction in Ig-enzyme complexes [2, 9]. \n \nComplex formation with IgA-type immunoglobulins was reported in 92% of the patients with macroamylasemia [2, 9]. Liver cirrhosis is known to be a condition that increases IgA production through the following mechanism: Serum albumin concentrations are greatly reduced by increased albumin degradation as well as decreased synthesis. To maintain plasma oncotic pressure, the shortage in albumin is compensated by a polyclonal increase in Igs. This polyclonal gammopathy involves all Igs such that an increase of IgA in the beta region shows beta-gamma bridging [10]. Although there is no information on the Ig subtypes that are involved in the formation of macroamylase, polyclonal gammopathy might contribute to an increased propensity between amylase and Ig to form macroenzymes. \n \nThe latent period for the clinical appearance of macroamylasemia varies from several weeks to months [2]. Hyperamylasemia persisted in our patient even though the symptoms and radiological findings of acute pancreatitis showed clinical improvement. Therefore, although macroamylasemia was diagnosed only a few weeks prior to presentation, it persisted even after the resolution of acute pancreatitis. \n \nTo avoid unnecessary laboratory tests, misdiagnosis, and overtreatment, it is essential to differentiate macroamylasemia from hyperamylasemia, particularly in patients without corroborating clinical evidence for hyperamylasemia. Therefore, we suggest that patients with macroamylasemia of unknown origin should be carefully assessed since they may have an underlying condition characterized by Ig overproduction even though they may present with persistent hyperamylasemia.","PeriodicalId":17890,"journal":{"name":"Korean Journal of Laboratory Medicine","volume":"31 2","pages":"98-100"},"PeriodicalIF":0.0000,"publicationDate":"2011-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.3343/kjlm.2011.31.2.98","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Laboratory Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3343/kjlm.2011.31.2.98","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
Accurate interpretation of elevated amylase levels is essential, especially for patients presenting with an overlapping pancreatic or liver disease or for patients with a history of these diseases [1]. In this study, we have described an unusual case of macroamylasemia that occurred immediately after acute pancreatitis. On March 9, 2010, a 56-yr-old Korean man was admitted to the emergency department because of confusion and delirium. He had previously been hospitalized for 4 months because of alcoholic cirrhosis and had been discharged 5 days prior to this admission. During the 4-month hospitalization, he had received treatment for esophageal variceal bleeding and acute pancreatitis. At that time, his serum amylase levels and lipase levels were 1,171 U/L and 298 U/L, respectively. Abdominal computed tomography images showed mild swelling of the pancreas and a cystic lesion (1.5 cm) in the pancreatic head (Fig. 1). The patient received therapy for acute pancreatitis. Although he showed improvement in symptoms and radiological findings at the time of discharge, on March 4, 2010, the serum amylase levels had increased to 1,882 U/L (Fig. 2). Five days later, the patient was readmitted because of altered mental status. Physical examinations revealed no abdominal pain and no rebound tenderness. The results of the blood biochemistry tests were as follows: total protein, 9.2 g/dL; albumin, 2.9 g/dL; amylase, 2,232 IU/L (25-125 IU/L); lipase, 61 IU/L (5.5-58 IU/L); total bilirubin, 2.39 mg/dL; direct bilirubin, 1.63 mg/dL; AST, 48 IU/L; ALT, 30 IU/L; alkaline phosphatase (ALP), 64 IU/L; gamma-glutamyl transpeptidase (GGT), 29 IU/L; and ammonia, 141 mg/dL. The serological tests yielded the following results: IgG, 3,850 mg/dL (700-1,600 mg/dL) and IgA, 664 mg/dL (70-400 mg/dL). After readmission, the urine amylase level was 54 IU/L (1-352 IU/L), and the amylase-creatinine clearance ratio (ACCR) was calculated to be 0.07%. Macroamylasemia was diagnosed on the basis of these findings. Serum amylase isoenzyme electrophoresis showed that the proportions of P-type and S-type amylases were 75.3% and 24.7%, respectively. Capillary serum protein electrophoresis revealed polyclonal gammopathy with a beta-gamma bridge pattern, which is a typical pattern in liver cirrhosis (Fig. 3). The patient's mental status returned to normal, and he is still in the hospital for continued management of liver cirrhosis.
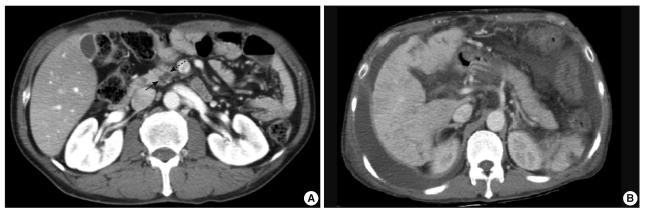
Fig. 1
Findings of abdominal computed tomography performed when the patient showed acute pancreatitis. A cystic lesion (arrows, 1.5 cm) in the pancreatic head region (A) and mild swelling of the pancreas (B) are observed.
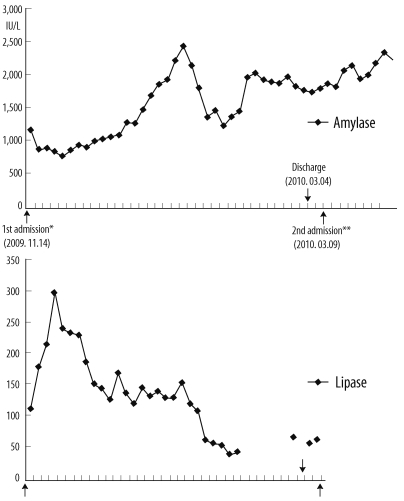
Fig. 2
Trends in the serum amylase and lipase levels from the time of diagnosis of acute pancreatitis (*) to the time of diagnosis of macroamylasemia (**). Serum amylase levels are high for about 4 months, while lipase levels fall near the upper reference limit. ...
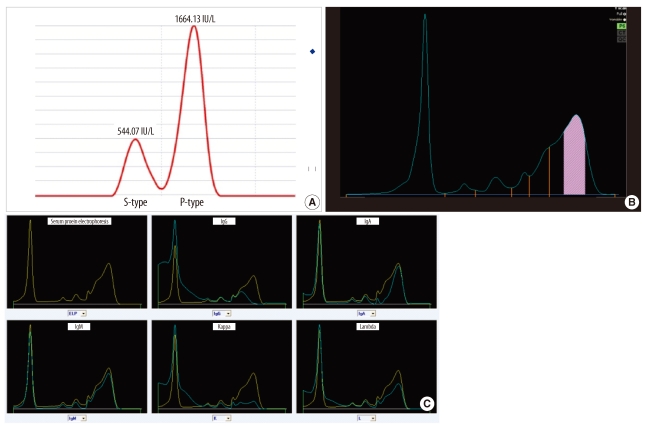
Fig. 3
Serum amylase isoenzyme electrophoresis (A) and capillary electrophoresis (B and C). (A) The P-type amylase level increased to 1,664.13 IU/L (75.30% of the total amylase concentration). The S-type amylase level is within the reference interval (545.87 ...
Macroamylasemia has been reported in 2.5% of the patients with hyperamylasemia and in 1% of the general population; approximately 0.4% of the cases in the general population occur in the West [2, 3]. Increased amylase and/or lipase activities were seen in 8% of the patients without pancreatic diseases [4]. In the previous reports, macroamylasemia was mainly reported in patients with disturbed humoral immunity, such as those with celiac disease, multiple myeloma, HIV infection, ulcerative colitis, and rheumatoid arthritis [2, 3, 5-8]. One of the predisposing conditions for macroamylasemia is a polyclonal increase in immunoglobulins (Ig). Some studies have reported that macroamylasemia may decrease or resolve when these underlying diseases are treated, and that the risk for autoimmune or lymphoproliferative diseases is higher in macroamylasemia with light-chain restriction in Ig-enzyme complexes [2, 9].
Complex formation with IgA-type immunoglobulins was reported in 92% of the patients with macroamylasemia [2, 9]. Liver cirrhosis is known to be a condition that increases IgA production through the following mechanism: Serum albumin concentrations are greatly reduced by increased albumin degradation as well as decreased synthesis. To maintain plasma oncotic pressure, the shortage in albumin is compensated by a polyclonal increase in Igs. This polyclonal gammopathy involves all Igs such that an increase of IgA in the beta region shows beta-gamma bridging [10]. Although there is no information on the Ig subtypes that are involved in the formation of macroamylase, polyclonal gammopathy might contribute to an increased propensity between amylase and Ig to form macroenzymes.
The latent period for the clinical appearance of macroamylasemia varies from several weeks to months [2]. Hyperamylasemia persisted in our patient even though the symptoms and radiological findings of acute pancreatitis showed clinical improvement. Therefore, although macroamylasemia was diagnosed only a few weeks prior to presentation, it persisted even after the resolution of acute pancreatitis.
To avoid unnecessary laboratory tests, misdiagnosis, and overtreatment, it is essential to differentiate macroamylasemia from hyperamylasemia, particularly in patients without corroborating clinical evidence for hyperamylasemia. Therefore, we suggest that patients with macroamylasemia of unknown origin should be carefully assessed since they may have an underlying condition characterized by Ig overproduction even though they may present with persistent hyperamylasemia.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
