Aaron W Pederson, Joseph K Salama, Daniel J Haraf, Mary Ellen Witt, Kerstin M Stenson, Louis Portugal, Tanguy Seiwert, Victoria M Villaflor, Ezra E W Cohen, Everett E Vokes, Elizabeth A Blair
{"title":"Adjuvant chemoradiotherapy for locoregionally advanced and high-risk salivary gland malignancies.","authors":"Aaron W Pederson, Joseph K Salama, Daniel J Haraf, Mary Ellen Witt, Kerstin M Stenson, Louis Portugal, Tanguy Seiwert, Victoria M Villaflor, Ezra E W Cohen, Everett E Vokes, Elizabeth A Blair","doi":"10.1186/1758-3284-3-31","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To report the outcomes of patients with locoregionally advanced and high- risk salivary gland malignancies treated with surgery followed by adjuvant chemoradiotherapy.</p><p><strong>Methods: </strong>From 09/1991 - 06/2007, 24 high-risk salivary gland cancer patients were treated with surgery, followed by adjuvant chemoradiotherapy for high-risk pathologic features including, perineural involvement, nodal involvement, positive margins, or T3/T4 tumors. Chemoradiotherapy was delivered for 4-6 alternating week cycles: the most common regimen, TFHX, consisted of 5 days paclitaxel (100 mg/m² on d1), infusional 5-fluorouracil (600 mg/m²/d × 5d), hydroxyurea (500 mg PO BID), and 1.5 Gy twice daily irradiation followed by a 9-day break without treatment.</p><p><strong>Results: </strong>Median follow-up was 42 months. The parotid gland was more frequently involved (n = 17) than minor (n = 4) or submandibular (n = 3) glands. The median radiation dose was 65 Gy (range 55-68 Gy). Acute treatment related toxicity included 46% grade 3 mucositis and 33% grade 3 hematologic toxicity. Six patients required feeding tubes during treatment. One patient progressed locally, 8 patients progressed distantly, and none progressed regionally. Five-year locoregional progression free survival was 96%. The 3 and 5 year overall survival was 79% and 59%, respectively. Long-term complications included persistent xerostomia (n = 5), esophageal stricture requiring dilatation (n = 1), and tempromandibular joint syndrome (n = 1).</p><p><strong>Conclusions: </strong>Surgical resection followed by adjuvant chemoradiotherapy results in promising locoregional control for high-risk salivary malignancy patients.</p>","PeriodicalId":49195,"journal":{"name":"Head and Neck Optical Diagnostics Society","volume":"3 ","pages":"31"},"PeriodicalIF":0.0000,"publicationDate":"2011-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1758-3284-3-31","citationCount":"48","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Head and Neck Optical Diagnostics Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1758-3284-3-31","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 48
Abstract
Background: To report the outcomes of patients with locoregionally advanced and high- risk salivary gland malignancies treated with surgery followed by adjuvant chemoradiotherapy.
Methods: From 09/1991 - 06/2007, 24 high-risk salivary gland cancer patients were treated with surgery, followed by adjuvant chemoradiotherapy for high-risk pathologic features including, perineural involvement, nodal involvement, positive margins, or T3/T4 tumors. Chemoradiotherapy was delivered for 4-6 alternating week cycles: the most common regimen, TFHX, consisted of 5 days paclitaxel (100 mg/m² on d1), infusional 5-fluorouracil (600 mg/m²/d × 5d), hydroxyurea (500 mg PO BID), and 1.5 Gy twice daily irradiation followed by a 9-day break without treatment.
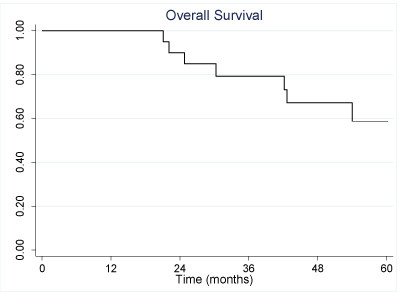
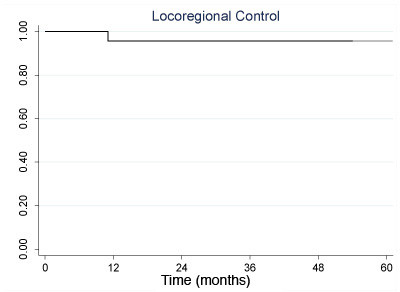
Results: Median follow-up was 42 months. The parotid gland was more frequently involved (n = 17) than minor (n = 4) or submandibular (n = 3) glands. The median radiation dose was 65 Gy (range 55-68 Gy). Acute treatment related toxicity included 46% grade 3 mucositis and 33% grade 3 hematologic toxicity. Six patients required feeding tubes during treatment. One patient progressed locally, 8 patients progressed distantly, and none progressed regionally. Five-year locoregional progression free survival was 96%. The 3 and 5 year overall survival was 79% and 59%, respectively. Long-term complications included persistent xerostomia (n = 5), esophageal stricture requiring dilatation (n = 1), and tempromandibular joint syndrome (n = 1).
Conclusions: Surgical resection followed by adjuvant chemoradiotherapy results in promising locoregional control for high-risk salivary malignancy patients.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
