Chung Hee Baek, Won Seok Yang, Kyung Sun Park, Duck Jong Han, Jae Berm Park, Su-Kil Park
{"title":"Infectious risks and optimal strength of maintenance immunosuppressants in rituximab-treated kidney transplantation.","authors":"Chung Hee Baek, Won Seok Yang, Kyung Sun Park, Duck Jong Han, Jae Berm Park, Su-Kil Park","doi":"10.1159/000337339","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rituximab, an anti-CD20 antibody, effectively depletes B lymphocytes. It is not clear whether the use of conventional doses of mycophenolate mofetil (MMF), methylprednisolone and tacrolimus as maintenance immunosuppression in rituximab-treated kidney transplantation is associated with increased risk.</p><p><strong>Methods: </strong>We retrospectively evaluated 67 patients who underwent HLA-sensitized or ABO-incompatible living donor kidney transplantation after one dose of rituximab (200 or 500 mg) (group 1). Eighty-seven kidney transplant recipients who did not require rituximab served as a control (group 2).</p><p><strong>Results: </strong>Cytomegalovirus infection (16.4 vs. 5.7%, p = 0.031) and pneumonia (9.0 vs. 1.1%, p = 0.043) occurred more often in group 1, and 2 patients of group 1 died of infection. The doses of methylprednisolone and tacrolimus levels of the two groups were not different. MMF dose was reduced when serious infection occurred. The doses of MMF (in grams/day) at the following times postoperatively were lower in group 1 than in group 2: 1 month: 1.26 ± 0.42 vs. 1.40 ± 0.39, p = 0.033; 3 months: 1.14 ± 0.51 vs. 1.36 ± 0.39, p = 0.011; 6 months: 1.07 ± 0.50 vs. 1.30 ± 0.42, p = 0.012; 1 year: 0.88 ± 0.52 vs. 1.19 ± 0.44, p = 0.009; 2 years: 0.69 ± 0.55 vs. 1.25 ± 0.49, p = 0.059, but the reduction of MMF doses did not increase the incidence of acute rejection in group 1 (4.5% in group 1 vs. 9.2% in group 2, p = 0.351). If patients who died with functioning graft were excluded, graft survival was 98.5% in group 1 and 100% in group 2.</p><p><strong>Conclusions: </strong>Serious infectious complications were increased in rituximab-treated kidney transplant recipients and it might be adequate to reduce the MMF dose from the early postoperative period.</p>","PeriodicalId":56356,"journal":{"name":"Nephron Extra","volume":"2 1","pages":"66-75"},"PeriodicalIF":0.0000,"publicationDate":"2012-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000337339","citationCount":"21","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephron Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000337339","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/3/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 21
Abstract
Background: Rituximab, an anti-CD20 antibody, effectively depletes B lymphocytes. It is not clear whether the use of conventional doses of mycophenolate mofetil (MMF), methylprednisolone and tacrolimus as maintenance immunosuppression in rituximab-treated kidney transplantation is associated with increased risk.
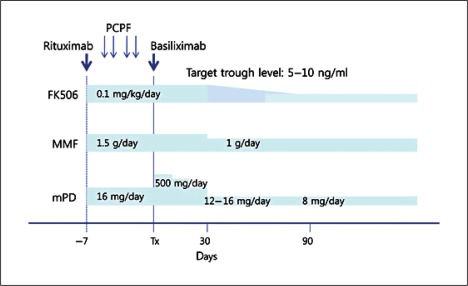
Methods: We retrospectively evaluated 67 patients who underwent HLA-sensitized or ABO-incompatible living donor kidney transplantation after one dose of rituximab (200 or 500 mg) (group 1). Eighty-seven kidney transplant recipients who did not require rituximab served as a control (group 2).
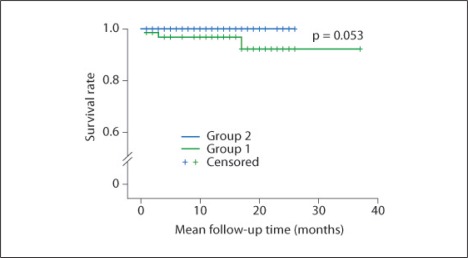
Results: Cytomegalovirus infection (16.4 vs. 5.7%, p = 0.031) and pneumonia (9.0 vs. 1.1%, p = 0.043) occurred more often in group 1, and 2 patients of group 1 died of infection. The doses of methylprednisolone and tacrolimus levels of the two groups were not different. MMF dose was reduced when serious infection occurred. The doses of MMF (in grams/day) at the following times postoperatively were lower in group 1 than in group 2: 1 month: 1.26 ± 0.42 vs. 1.40 ± 0.39, p = 0.033; 3 months: 1.14 ± 0.51 vs. 1.36 ± 0.39, p = 0.011; 6 months: 1.07 ± 0.50 vs. 1.30 ± 0.42, p = 0.012; 1 year: 0.88 ± 0.52 vs. 1.19 ± 0.44, p = 0.009; 2 years: 0.69 ± 0.55 vs. 1.25 ± 0.49, p = 0.059, but the reduction of MMF doses did not increase the incidence of acute rejection in group 1 (4.5% in group 1 vs. 9.2% in group 2, p = 0.351). If patients who died with functioning graft were excluded, graft survival was 98.5% in group 1 and 100% in group 2.
Conclusions: Serious infectious complications were increased in rituximab-treated kidney transplant recipients and it might be adequate to reduce the MMF dose from the early postoperative period.
期刊介绍:
An open-access subjournal to Nephron. ''Nephron EXTRA'' publishes additional high-quality articles that cannot be published in the main journal ''Nephron'' due to space limitations.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
