{"title":"Fibrosis in the kidney: is a problem shared a problem halved?","authors":"Tim D Hewitson","doi":"10.1186/1755-1536-5-S1-S14","DOIUrl":null,"url":null,"abstract":"<p><p>Fibrotic disorders are commonplace, take many forms and can be life-threatening. No better example of this exists than the progressive fibrosis that accompanies all chronic renal disease. Renal fibrosis is a direct consequence of the kidney's limited capacity to regenerate after injury. Renal scarring results in a progressive loss of renal function, ultimately leading to end-stage renal failure and a requirement for dialysis or kidney transplantation. Although it manifests itself histologically as an increase in extracellular matrix, we know that the histological appearance can be caused by a de novo synthesis of matrix (primarily collagen), or a disproportionate loss of renal parenchyma. In both cases the process depends on a resident mesenchymal cell, the so-called myofibroblast, and is independent of disease etiology. Potentially we can ameliorate fibrosis, either indirectly by modifying the environment the kidney functions in, or more directly by interfering with activation and function of myofibroblasts. However, while renal fibrosis shares many features in common with the wound healing response in other organs, we also recognise that the consequences can be highly kidney specific. This review highlights the similarities and differences between this process in the kidney and other organs, and considers the therapeutic implications. </p>","PeriodicalId":12264,"journal":{"name":"Fibrogenesis & Tissue Repair","volume":"5 Suppl 1","pages":"S14"},"PeriodicalIF":0.0000,"publicationDate":"2012-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1755-1536-5-S1-S14","citationCount":"71","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Fibrogenesis & Tissue Repair","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1755-1536-5-S1-S14","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 71
Abstract
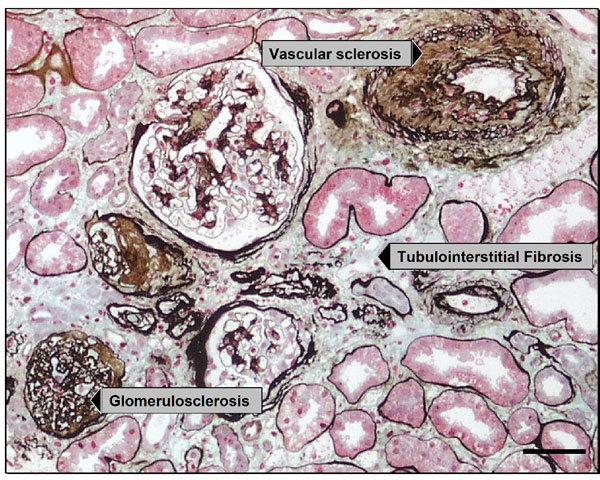
Fibrotic disorders are commonplace, take many forms and can be life-threatening. No better example of this exists than the progressive fibrosis that accompanies all chronic renal disease. Renal fibrosis is a direct consequence of the kidney's limited capacity to regenerate after injury. Renal scarring results in a progressive loss of renal function, ultimately leading to end-stage renal failure and a requirement for dialysis or kidney transplantation. Although it manifests itself histologically as an increase in extracellular matrix, we know that the histological appearance can be caused by a de novo synthesis of matrix (primarily collagen), or a disproportionate loss of renal parenchyma. In both cases the process depends on a resident mesenchymal cell, the so-called myofibroblast, and is independent of disease etiology. Potentially we can ameliorate fibrosis, either indirectly by modifying the environment the kidney functions in, or more directly by interfering with activation and function of myofibroblasts. However, while renal fibrosis shares many features in common with the wound healing response in other organs, we also recognise that the consequences can be highly kidney specific. This review highlights the similarities and differences between this process in the kidney and other organs, and considers the therapeutic implications.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
