Improved Insulin Sensitivity during Pioglitazone Treatment Is Associated with Changes in IGF-I and Cortisol Secretion in Type 2 Diabetes and Impaired Glucose Tolerance.
Lisa Arnetz, Neda Rajamand Ekberg, Charlotte Höybye, Kerstin Brismar, Michael Alvarsson
{"title":"Improved Insulin Sensitivity during Pioglitazone Treatment Is Associated with Changes in IGF-I and Cortisol Secretion in Type 2 Diabetes and Impaired Glucose Tolerance.","authors":"Lisa Arnetz, Neda Rajamand Ekberg, Charlotte Höybye, Kerstin Brismar, Michael Alvarsson","doi":"10.1155/2013/148497","DOIUrl":null,"url":null,"abstract":"<p><p>Background. Hypercortisolism and type 2 diabetes (T2D) share clinical characteristics. We examined pioglitazone's effects on the GH-IGF-I and HPA axes in men with varying glucose intolerance. Methods. 10 men with T2D and 10 with IGT received pioglitazone 30-45 mg for 12 weeks. OGTT with microdialysis in subcutaneous adipose tissue and 1 μg ACTH-stimulation test were performed before and after. Glucose, insulin, IGF-I, IGFBP1, and interstitial measurements were analyzed during the OGTT. Insulin sensitivity was estimated using HOMA-IR. Results. HOMA-IR improved in both groups. IGF-I was initially lower in T2D subjects (P = 0.004) and increased during treatment (-1.4 ± 0.5 to -0.5 ± 0.4 SD; P = 0.007); no change was seen in IGT (0.4 ± 39 SD before and during treatment). Fasting glycerol decreased in T2D (P = 0.038), indicating reduced lipolysis. Fasting cortisol decreased in T2D (400 ± 30 to 312 ± 25 nmol/L; P = 0.041) but increased in IGT (402 ± 21 to 461 ± 35 nmol/L; P = 0.044). Peak cortisol was lower in T2D during treatment (599 ± 32 to 511 ± 43, versus 643 ± 0.3 to 713 ± 37 nmol/L in IGT; P = 0.007). Conclusions. Pioglitazone improved adipose tissue and liver insulin sensitivity in both groups. This may explain increased IGF-I in T2D. Pioglitazone affected cortisol levels in both groups but differently, suggesting different mechanisms for improving insulin sensitivity between T2D and IGT.</p>","PeriodicalId":89576,"journal":{"name":"ISRN endocrinology","volume":"2013 ","pages":"148497"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2013/148497","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2013/148497","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
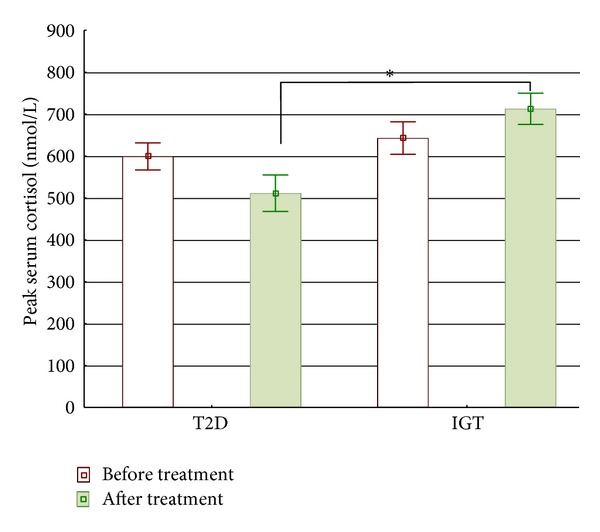
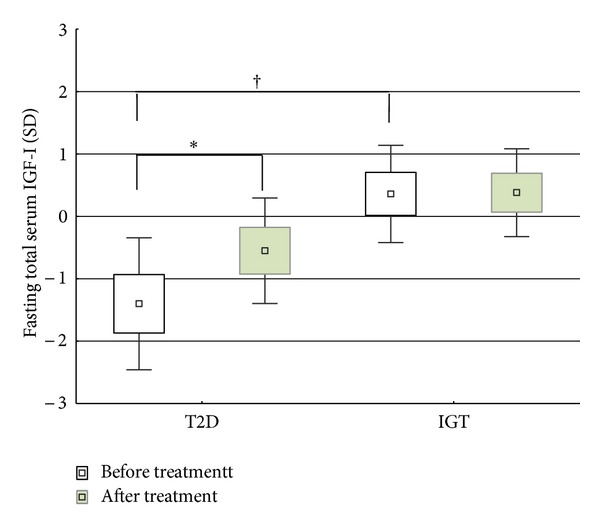
Background. Hypercortisolism and type 2 diabetes (T2D) share clinical characteristics. We examined pioglitazone's effects on the GH-IGF-I and HPA axes in men with varying glucose intolerance. Methods. 10 men with T2D and 10 with IGT received pioglitazone 30-45 mg for 12 weeks. OGTT with microdialysis in subcutaneous adipose tissue and 1 μg ACTH-stimulation test were performed before and after. Glucose, insulin, IGF-I, IGFBP1, and interstitial measurements were analyzed during the OGTT. Insulin sensitivity was estimated using HOMA-IR. Results. HOMA-IR improved in both groups. IGF-I was initially lower in T2D subjects (P = 0.004) and increased during treatment (-1.4 ± 0.5 to -0.5 ± 0.4 SD; P = 0.007); no change was seen in IGT (0.4 ± 39 SD before and during treatment). Fasting glycerol decreased in T2D (P = 0.038), indicating reduced lipolysis. Fasting cortisol decreased in T2D (400 ± 30 to 312 ± 25 nmol/L; P = 0.041) but increased in IGT (402 ± 21 to 461 ± 35 nmol/L; P = 0.044). Peak cortisol was lower in T2D during treatment (599 ± 32 to 511 ± 43, versus 643 ± 0.3 to 713 ± 37 nmol/L in IGT; P = 0.007). Conclusions. Pioglitazone improved adipose tissue and liver insulin sensitivity in both groups. This may explain increased IGF-I in T2D. Pioglitazone affected cortisol levels in both groups but differently, suggesting different mechanisms for improving insulin sensitivity between T2D and IGT.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
