{"title":"LACE+ index: extension of a validated index to predict early death or urgent readmission after hospital discharge using administrative data.","authors":"Carl van Walraven, Jenna Wong, Alan J Forster","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Death or urgent readmission after hospital discharge is a common adverse event that can be used to compare outcomes of care between institutions. To accurately adjust for risk and to allow for interhospital comparisons of readmission rates, we used administrative data to derive and internally validate an extension of the LACE index, a previously validated index for 30-day death or urgent readmission.</p><p><strong>Methods: </strong>We randomly selected 500 000 medical and surgical patients discharged to the community from any Ontario hospital between 1 April 2003 and 31 March 2009. We derived a logistic regression model on 250 000 randomly selected patients from this group and modified the final model into an index scoring system, the LACE+ index. We internally validated the LACE+ index using data from the remaining 250 000 patients and compared its performance with that of the original LACE index.</p><p><strong>Results: </strong>Within 30 days of discharge to the community, 33 825 (6.8%) of the patients had died or had been urgently readmitted. In addition to the variables included in the LACE index (length of stay in hospital [L], acuity of admission [A], comorbidity [C] and emergency department utilization in the 6 months before admission [E]), the LACE+ index incorporated patient age and sex, teaching status of the discharge hospital, acute diagnoses and procedures performed during the index admission, number of days on alternative level of care during the index admission, and number of elective and urgent admissions to hospital in the year before the index admission. The LACE+ index was highly discriminative (C statistic 0.771, 95% confidence interval 0.767-0.775), was well calibrated across most of its range of scores and had a model performance that exceeded that of the LACE index.</p><p><strong>Interpretation: </strong>The LACE+ index can be used to predict the risk of postdischarge death or urgent readmission on the basis of administrative data for the Ontario population. Its performance exceeds that of the LACE index, and it allows analysts to accurately estimate the risk of important postdischarge outcomes.</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"6 3","pages":"e80-90"},"PeriodicalIF":0.0000,"publicationDate":"2012-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/28/OpenMed-06-e80.PMC3659212.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/1/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Death or urgent readmission after hospital discharge is a common adverse event that can be used to compare outcomes of care between institutions. To accurately adjust for risk and to allow for interhospital comparisons of readmission rates, we used administrative data to derive and internally validate an extension of the LACE index, a previously validated index for 30-day death or urgent readmission.
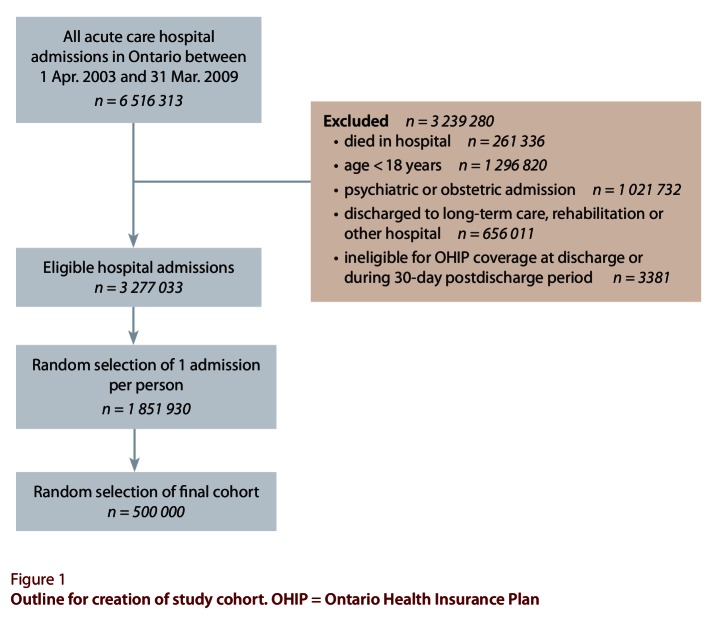
Methods: We randomly selected 500 000 medical and surgical patients discharged to the community from any Ontario hospital between 1 April 2003 and 31 March 2009. We derived a logistic regression model on 250 000 randomly selected patients from this group and modified the final model into an index scoring system, the LACE+ index. We internally validated the LACE+ index using data from the remaining 250 000 patients and compared its performance with that of the original LACE index.
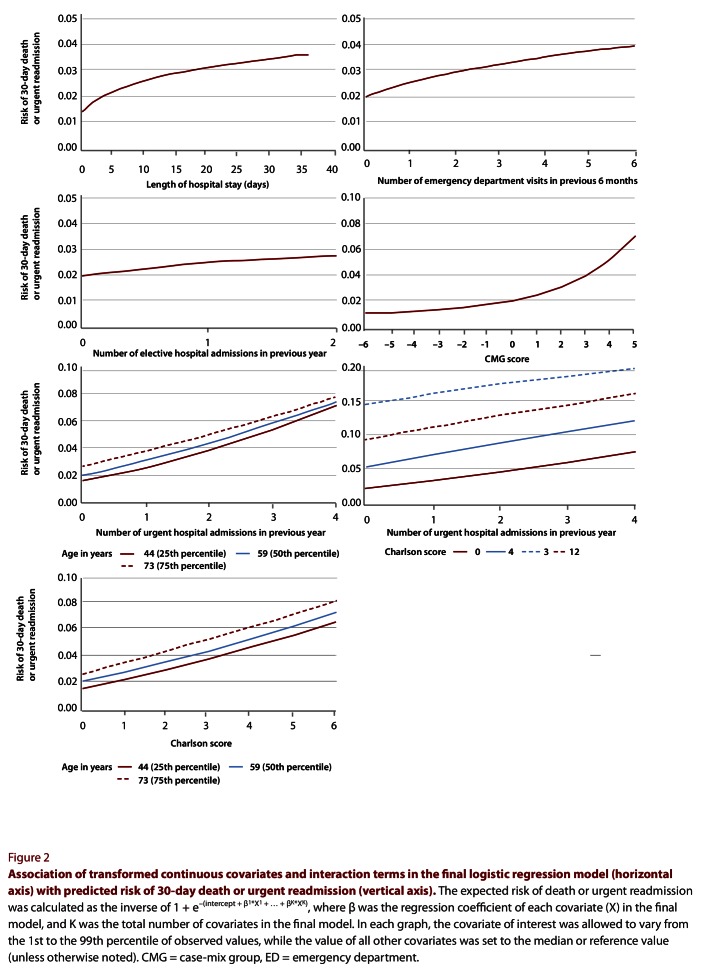
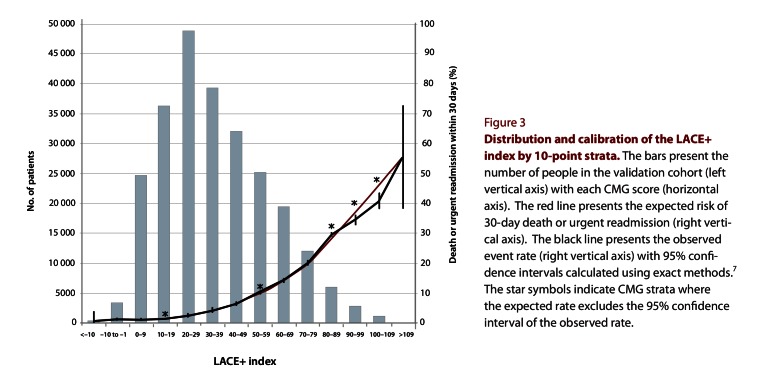
Results: Within 30 days of discharge to the community, 33 825 (6.8%) of the patients had died or had been urgently readmitted. In addition to the variables included in the LACE index (length of stay in hospital [L], acuity of admission [A], comorbidity [C] and emergency department utilization in the 6 months before admission [E]), the LACE+ index incorporated patient age and sex, teaching status of the discharge hospital, acute diagnoses and procedures performed during the index admission, number of days on alternative level of care during the index admission, and number of elective and urgent admissions to hospital in the year before the index admission. The LACE+ index was highly discriminative (C statistic 0.771, 95% confidence interval 0.767-0.775), was well calibrated across most of its range of scores and had a model performance that exceeded that of the LACE index.
Interpretation: The LACE+ index can be used to predict the risk of postdischarge death or urgent readmission on the basis of administrative data for the Ontario population. Its performance exceeds that of the LACE index, and it allows analysts to accurately estimate the risk of important postdischarge outcomes.
 分享
分享



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
