Clinical and cost effectiveness of switching asthma patients from fluticasone-salmeterol to extra-fine particle beclometasone-formoterol: a retrospective matched observational study of real-world patients.
David Price, Iain Small, John Haughney, Dermot Ryan, Kevin Gruffydd-Jones, Federico Lavorini, Tim Harris, Annie Burden, Jeremy Brockman, Christine King, Alberto Papi
{"title":"Clinical and cost effectiveness of switching asthma patients from fluticasone-salmeterol to extra-fine particle beclometasone-formoterol: a retrospective matched observational study of real-world patients.","authors":"David Price, Iain Small, John Haughney, Dermot Ryan, Kevin Gruffydd-Jones, Federico Lavorini, Tim Harris, Annie Burden, Jeremy Brockman, Christine King, Alberto Papi","doi":"10.4104/pcrj.2013.00088","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Efficacy trials suggest that extra-fine particle beclometasone dipropionate-formoterol (efBDP-FOR) is comparable to fluticasone propionate-salmeterol (FP-SAL) in preventing asthma exacerbations at a clinically equivalent dosage. However, switching from FP-SAL to efBDP-FOR has not been evaluated in real-world asthma patients.</p><p><strong>Aims: </strong>The REACH (Real-world Effectiveness in Asthma therapy of Combination inHalers) study investigated the clinical and cost effectiveness of switching typical asthma patients from FP-SAL to efBDP-FOR.</p><p><strong>Methods: </strong>A retrospective matched (1:3) observational study of 1,528 asthma patients aged 18-80 years from clinical practice databases was performed. Patients remaining on FP-SAL (n=1,146) were compared with those switched to efBDP-FOR at an equivalent or lower inhaled corticosteroid (ICS) dosage (n=382). Clinical and economic outcomes were compared between groups for the year before and after the switch. Non-inferiority (at least equivalence) of efBDP-FOR was tested against FP-SAL by comparing exacerbation rates during the outcome year.</p><p><strong>Results: </strong>efBDP-FOR was non-inferior to FP-SAL (adjusted exacerbation rate ratio 1.01 (95% CI 0.74 to 1.37)). Switching to efBDP-FOR resulted in significantly better (p<0.05) odds of achieving overall asthma control (no asthma-related hospitalisations, bronchial infections, or acute oral steroids; salbutamol ≤200μg/day) and lower daily short-acting β2-agonist usage at a lower daily ICS dosage (mean -130μg/day FP equivalents; p<0.001). It also reduced mean asthma-related healthcare costs by £93.63/patient/year (p<0.001).</p><p><strong>Conclusions: </strong>Asthma patients may be switched from FP-SAL to efBDP-FOR at an equivalent or lower ICS dosage with no reduction in clinical effectiveness but a significant reduction in cost.</p>","PeriodicalId":48998,"journal":{"name":"Primary Care Respiratory Journal","volume":"22 4","pages":"439-48"},"PeriodicalIF":0.0000,"publicationDate":"2013-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4104/pcrj.2013.00088","citationCount":"41","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Primary Care Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4104/pcrj.2013.00088","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 41
Abstract
Background: Efficacy trials suggest that extra-fine particle beclometasone dipropionate-formoterol (efBDP-FOR) is comparable to fluticasone propionate-salmeterol (FP-SAL) in preventing asthma exacerbations at a clinically equivalent dosage. However, switching from FP-SAL to efBDP-FOR has not been evaluated in real-world asthma patients.
Aims: The REACH (Real-world Effectiveness in Asthma therapy of Combination inHalers) study investigated the clinical and cost effectiveness of switching typical asthma patients from FP-SAL to efBDP-FOR.
Methods: A retrospective matched (1:3) observational study of 1,528 asthma patients aged 18-80 years from clinical practice databases was performed. Patients remaining on FP-SAL (n=1,146) were compared with those switched to efBDP-FOR at an equivalent or lower inhaled corticosteroid (ICS) dosage (n=382). Clinical and economic outcomes were compared between groups for the year before and after the switch. Non-inferiority (at least equivalence) of efBDP-FOR was tested against FP-SAL by comparing exacerbation rates during the outcome year.
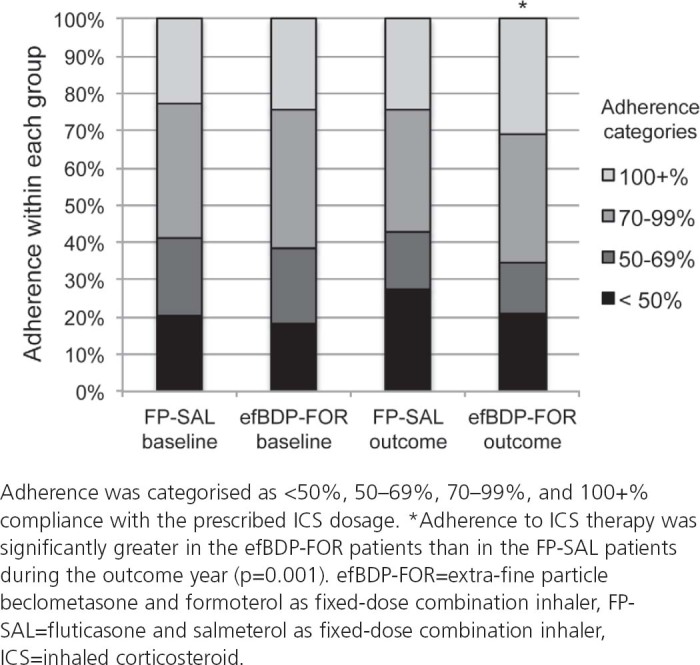
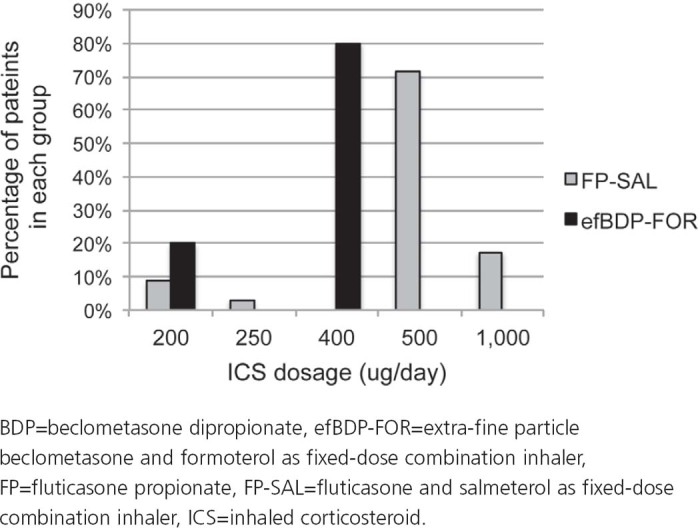
Results: efBDP-FOR was non-inferior to FP-SAL (adjusted exacerbation rate ratio 1.01 (95% CI 0.74 to 1.37)). Switching to efBDP-FOR resulted in significantly better (p<0.05) odds of achieving overall asthma control (no asthma-related hospitalisations, bronchial infections, or acute oral steroids; salbutamol ≤200μg/day) and lower daily short-acting β2-agonist usage at a lower daily ICS dosage (mean -130μg/day FP equivalents; p<0.001). It also reduced mean asthma-related healthcare costs by £93.63/patient/year (p<0.001).
Conclusions: Asthma patients may be switched from FP-SAL to efBDP-FOR at an equivalent or lower ICS dosage with no reduction in clinical effectiveness but a significant reduction in cost.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
