Mohamed Ghazaly, Mohamad T Badawy, Hosam El-Din Soliman, Magdy El-Gendy, Tarek Ibrahim, Brian R Davidson
{"title":"Venous Outflow Reconstruction in Adult Living Donor Liver Transplant: Outcome of a Policy for Right Lobe Grafts without the Middle Hepatic Vein.","authors":"Mohamed Ghazaly, Mohamad T Badawy, Hosam El-Din Soliman, Magdy El-Gendy, Tarek Ibrahim, Brian R Davidson","doi":"10.1155/2013/280857","DOIUrl":null,"url":null,"abstract":"<p><p>Introduction. The difficulty and challenge of recovering a right lobe graft without MHV drainage is reconstructing the outflow tract of the hepatic veins. With the inclusion or the reconstruction of the MHV, early graft function is satisfactory. The inclusion of the MHV or not in the donor's right lobectomy should be based on sound criteria to provide adequate functional liver mass for recipient, while keeping risk to donor to the minimum. Objective. Reviewing the results of a policy for right lobe grafts transplant without MHV and analyzing methods of venous reconstruction related to outcome. Materials and Methods. We have two groups Group A (with more than one HV anast.) (n = 16) and Group B (single HV anast.) (n = 24). Both groups were compared regarding indications for reconstruction, complications, and operative details and outcomes, besides describing different modalities used for venous reconstruction. Results. Significant increase in operative details time in Group A. When comparison came to complications and outcomes in terms of laboratory findings and overall hospital stay, there were no significant differences. Three-month and one-year survival were better in Group A. Conclusion. Adult LDLT is safely achieved with better outcome to recipients and donors by recovering the right lobe without MHV, provided that significant MHV tributaries (segments V, VIII more than 5 mm) are reconstructed, and any accessory considerable inferior right hepatic veins (IRHVs) or superficial RHVs are anastomosed. </p>","PeriodicalId":77165,"journal":{"name":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","volume":"2013 ","pages":"280857"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2013/280857","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HPB surgery : a world journal of hepatic, pancreatic and biliary surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2013/280857","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/12/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 7
Abstract
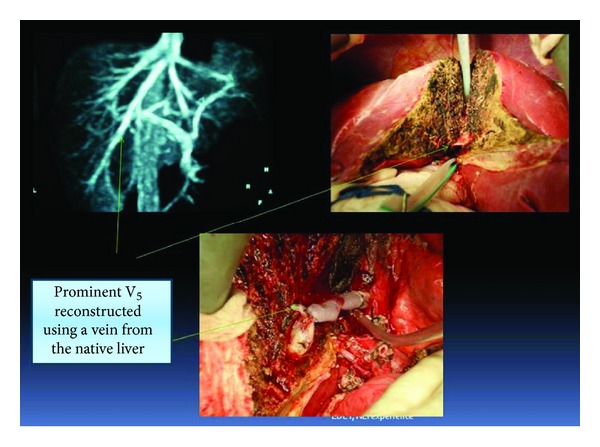
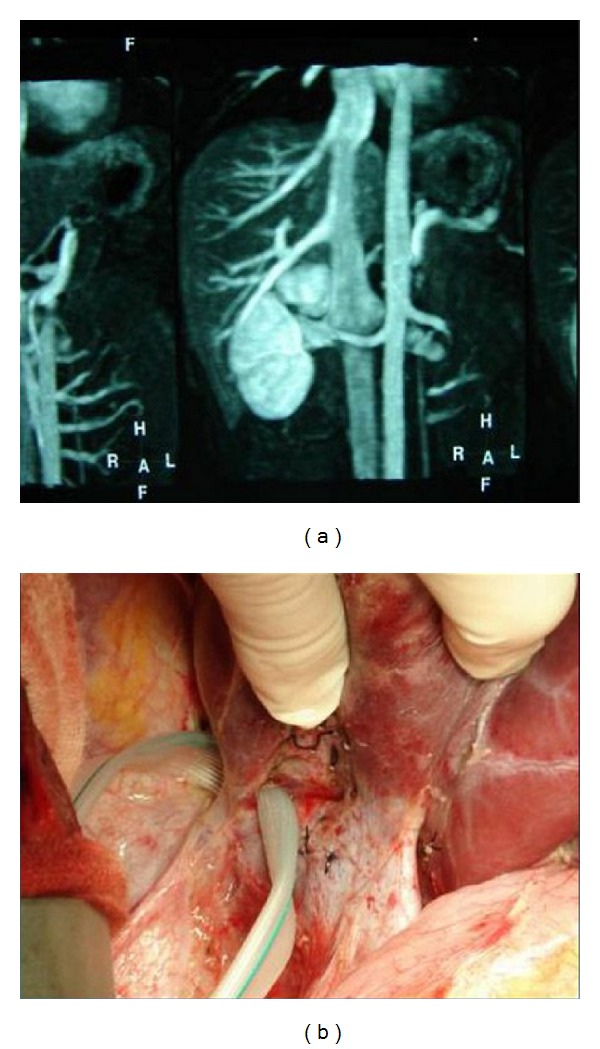
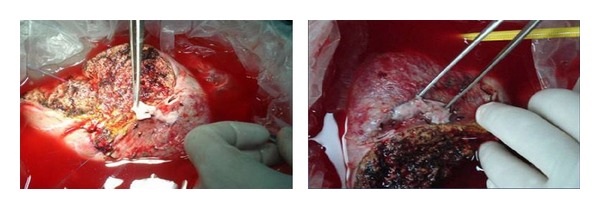
Introduction. The difficulty and challenge of recovering a right lobe graft without MHV drainage is reconstructing the outflow tract of the hepatic veins. With the inclusion or the reconstruction of the MHV, early graft function is satisfactory. The inclusion of the MHV or not in the donor's right lobectomy should be based on sound criteria to provide adequate functional liver mass for recipient, while keeping risk to donor to the minimum. Objective. Reviewing the results of a policy for right lobe grafts transplant without MHV and analyzing methods of venous reconstruction related to outcome. Materials and Methods. We have two groups Group A (with more than one HV anast.) (n = 16) and Group B (single HV anast.) (n = 24). Both groups were compared regarding indications for reconstruction, complications, and operative details and outcomes, besides describing different modalities used for venous reconstruction. Results. Significant increase in operative details time in Group A. When comparison came to complications and outcomes in terms of laboratory findings and overall hospital stay, there were no significant differences. Three-month and one-year survival were better in Group A. Conclusion. Adult LDLT is safely achieved with better outcome to recipients and donors by recovering the right lobe without MHV, provided that significant MHV tributaries (segments V, VIII more than 5 mm) are reconstructed, and any accessory considerable inferior right hepatic veins (IRHVs) or superficial RHVs are anastomosed.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
